Neck Vein Examination & Wave Forms
The jugular venous exam is an important aspect of assessing a patient's volume status, especially in patients with heart failure, liver failure and kidney failure. Both elevation of the neck veins and the variations of the neck vein waveforms share valuable information about a patient's diagnosis.
How to Measure the Jugular Venous Pressure (JVP)
- Get the patient to relax, raise the bed so you are not straining.
- Take the pillow away; the waveforms are often better seen with the head lying directly against the examining table/bed.
- Position the neck until you have the best view.
- If you make sure the room is well lit, there is no need for shining a flashlight, penlight or other direct light.
- Make your first goal just to see a pulsation, and then decide if it is arterial or venous by applying the following criteria to identify venous waves:
- Venous wave is bifid, flicking like a snake's tongue.
- It rises when you lower the head of the bed and sinks when you raise the head of the bed.
- It changes with respiration, sinking into the chest with inspiration.
- It is not palpable.
- It is fine to use the external jugular vein, as long as you can see clear wave forms in it.
- Commonly, a prominent pulsation is mistaken for that of the carotid artery rather than of the JVP. To differentiate, press on the RUQ while watching the neck. The JVP should rise in all individuals with this maneuver; whereas a carotid pulsation should not change.
- The JVP can be assessed on either the right or left. On occasion (musculoskeletal anatomy, venous clots) the pulsations can only be visualized on one side. If you cannot clearly define the JVP on the right internal jugular, examine the left.
- If you cannot determine the JVP, report the exam as "JVP not visualized" rather than "no JVD" (which implies that the JVP was visualized and is not elevated).
Once you have determined that you are seeing the venous waves then measure the jugular venous pressure:
- Identify JVP at the highest point of pulsation
- Extend card or ruler horizontally from highest pulsation point , cross with ruler placed on the sternal angle (Angle of Louis), (let's say it was 8cm).
- Add 5 cm (to get to the center of the atrium) and then report the JVP as "the jugular venous pressure was 13 cm of water" (not mercury).
Understanding the Jugular Venous Waveform
Normal Jugular Venous Waveforms
There are two positive waves 'a' and 'v', one occurring just before the first heart sound or the carotid impulse, and one just after. When the heart rate is 80 or less, they are fairly easy to time, but if the heart rate is fast, then you may need to auscultate while you observe.
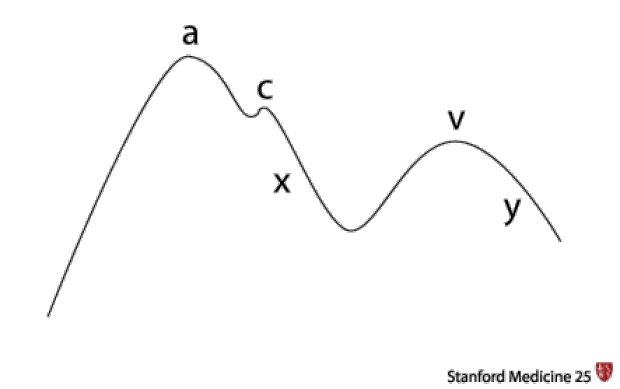
"A" wave: atrial contraction (ABSENT in atrial fibrillation)
"C" wave: ventricular contraction (tricuspid bulges). YOU WON'T SEE THIS
"X" descent: atrial relaxation
"V" wave: atrial venous filling (occurs at same of time of ventricular contraction)
"Y" descent: ventricular filling (tricuspid opens)
Abnormal Jugular Venous Waveforms
Elevated "a" wave
- Resistance to right atrial emptying, may occur at or beyond the tricuspid valve. Examples include:
- Pulmonary Hypertension
- Rheumatic tricuspid stenosis
- Right atrial mass or thrombus
Cannon "a" wave
- Large positive venous pulse during "a" wave. It occurs when an atrium contracts against a closed tricuspid valve during AV dissociation. Examples include:
- Premature atrial/junctional/ventricular beats
- Complete atrio-ventricular (AV) block
- Ventricular tachycardia
Absent "a" wave
- No atrial contraction, common to atrial fibrillation.
Elevated "v" wave
- Tricuspid regurgitation is the most common cause (Lancisi sign).
- The ventricle contracts and if the tricuspid valve does not close well, a jet of blood shoots into the right atrium.
- Tricuspid regurgitation, if significant, will be accompanied by a pulsatile liver (feel over the lower costal margin).
- You will also hear the murmur of tricuspid regurgitation—a pansystolic murmur that increases on inspiration.
Other signs:
- Kussmaul's sign: neck veins rise in inspiration rather than fall—often a sign of pericardial tamponade or right heart failure (acute right ventricular myocardial infarction)
- Friedrich's sign: exaggerated "x" wave or diastolic collapse of the neck veins from constrictive pericarditis.
Measuring Central Venous Pressure Using a Patient's Arm
Consult the Expert
Dr. Ronald Witteles
Dr. Ronald Witteles is certified in Internal Medicine and Cardiology. He serves as the Stanford Internal Medicine Program Director, Associate Director of the CCU and Co-Director, Stanford Amyloid Center.
Clinical Pearl
The sternal angle (Angle of Louis) is the most popular reference point to use because it remains approximately 5 cm above right atrium regardless of the patient's position. The clavicle can also be used as a reference point, however it will change with position. In the upright position, the clavicle is approximately 10 cm above the right atrium.
Key Learning Points
- Learn best technique to measure the jugular venous pressure
- Examine jugular venous wave forms for abnormalities
Related to Neck Vein Examination & Wave Forms
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam