Pupillary Responses
The pupil has tight neurological control and abnormalities of this control correlate with underlying diagnoses. The exam and those diagnoses are covered here.
Introduction to Pupillary Responses
There are a handful of pupillary abnormalities that every clinician should know. Here we review the basic physiology then describe these abnormal pupillary responses and how to find them.
Pupillary Control: The Basics
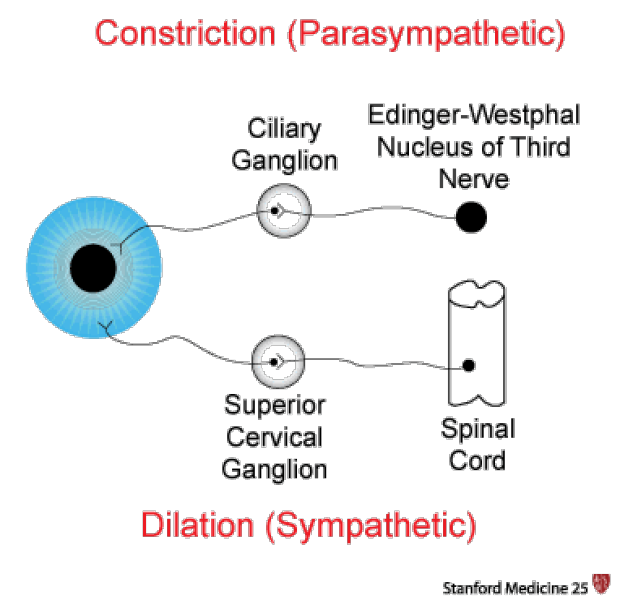
The physiology behind a "normal" pupillary constriction is a balance between the sympathetic and parasympathetic nervous systems.
Parasympathetic innervation leads to pupillary constriction. A circular muscle called the sphincter pupillae accomplishes this task. The fibers of the sphincter pupillae encompass the pupil. The pathway of pupillary constriction begins at the Edinger-Westphal nucleus near the occulomotor nerve nucleus. The fibers enter the orbit with CNIII nerve fibers and ultimately synapse at the cilliary ganglion.
Sympathetic innervation leads to pupillary dilation. Dilation is controlled by the dilator pupillae, a group of muscles in the peripheral 2/3 of the iris. Sympathetic innervation begins at the cortex with the first synapse at the cilliospinal center (also known as Budge's center after German physiologist Julius Ludwig Budge). Post synaptic neurons travel down all the way through the brain stem and finally exit through the cervical sympathetic chain and the superior cervical ganglion. They synapse at the superior cervical ganglion where third-order neurons travel through the carotid plexus and enter into the orbit through the first division of the trigeminal nerve.
Performing the Exam for Pupillary Responses
When performing a pupillary exam, it sometimes helps to illuminate pupils indirectly from the side, so you can actually see what is happening.
- Observe the pupil size and shape at rest, looking for anisocoria (one pupil larger than the other)
- Observe the direct response (constriction of the illuminated pupil)
- Observe the consensual response (constriction of the opposite pupil)
- Repeat with the opposite pupil
- Check for accommodation (constriction of pupil when viewing a close object)
Abnormal Pupillary Responses
Anisocoria
Refers to the asymmetric sizes of pupils
Physiologic anisocoria can is very common and a normal variant in up to 20% of the population. The variation should be no more than 1mm and both eyes should react to light normally.
Can be dangerous if a manifestation Horner's syndrome (e.g. carotid dissection) or from damage to the third nerve (e.g. aneurysmal expansion)
Consider further workup such as imaging if anisocoria is suspected to be from a pathologic process
Relative Afferent Pupillary Defect (RAPD, Marcus Gunn Pupil)
An RAPD is a defect in the direct response. It is due to damage inoptic nerve or severe retinal disease.
It is important to be able to differentiate whether a patient is complaining of decreased vision from an ocular problem such as cataract or from a defect of the optic nerve. If an optic nerve lesion is present the affected pupil will not constrict to light when light is shone in the that pupil during the swinging flashlight test. However, it will constrict if light is shone in the other eye (consensual response). The swinging flashlight test is helpful in separating these two etiologies as only patients with optic nerve damage will have a positive RAPD.
Swinging Flashlight Test:
Swing a light back and forth in front of the two pupils and compare the reaction to stimulation in both eyes.
When light reaches a pupil there should be a normal direct and consensual response.
An RAPD is diagnosed by observing paradoxical dilatation when light is directly shone in the affected pupil after being shown in the healthy pupild to be from a pathologic process

This decrease in constriction or widening of the pupil is due to reduced stimulation of the visual pathway by the pupil on the affected side. By not being able to relay the intensity of the light as accurately as the healthy pupil and visual pathway, the diseased side causes the visual pathway to mistakenly respond to the decrease in stimulation as if the flashlight itself were less luminous. This explains the healthy eye is able to undergo both direct and consensual dilatation seen on the swinging flashlight test.
Some causes of a RAPD include:
- optic neuritis
- ischemic optic disease or retinal disease
- severe glaucoma causing trauma to optic nerve
- direct optic nerve damage (trauma, radiation, tumor)
- retinal detachment
- very severe macular degeneration
- retinal infection (CMV, herpes)
Adie's (Tonic) Pupil
Common in women in the 3rd/4th decade of life (but also can be present in men)
Either no or sluggish response to light (both direct and consensual responses)
Thought to be caused from denervation in the postganglionic parasympathetic nerve
Associated with Holmes-Adie syndrome described with Adie's pupil and absent deep tendon reflexes
Overall, this is a benign process (including Holmes-Adie syndrome)
Argyll Robertson Pupil
This lesion is a hallmark of tertiary neurosyphillis
Pupils will NOT constrict to light but they WILL constrict with accommodation
Pupils are small at baseline and usually both involved (although degree may be asymmetrical)
Horner's Syndrome
Loss of sympathetic innervation causing the clinical triad of:
- Ptosis (drooping eyelid): The superior tarsal muscle requires sympathetic innervation to keep the eyelid retracted
- Miosis (pupillary constriction): A loss of sympathetic input causes unopposed parasympathetic stimulation which leads to pupillary constriction. This degree of miosis may be subtle and require a dark room.
- Anhidrosis (decreased sweating): Also caused by a loss of sympathetic activity. The pattern of anihidrosis may help identify the lesion. Anhidrosis of the entire face is often associated with a lesion at the level of the carotid artery. Partial anhidrosis involving only the medial aspect of the forehead ipsilateral side of the nose is associated with a lesion distal to the carotid bulb.
Causes of Horner's Syndrome include:
- carotid artery dissection
- pancoast tumors, nasopharyngial tumors
- lymphoproliferative disorders
- brachial plexus injury
- cavernous sinus thrombosis
- fibromuscular dysplasia
Marcus Gunn Pupil
For information on the Marcus Gunn pupil, click here.
Key Learning Points
- Learn abnormal pupillary responses and how to find them
Related to Pupillary Responses
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam