What Is The Specific Cause of This Patient’s Clubbing?
June 3, 2015
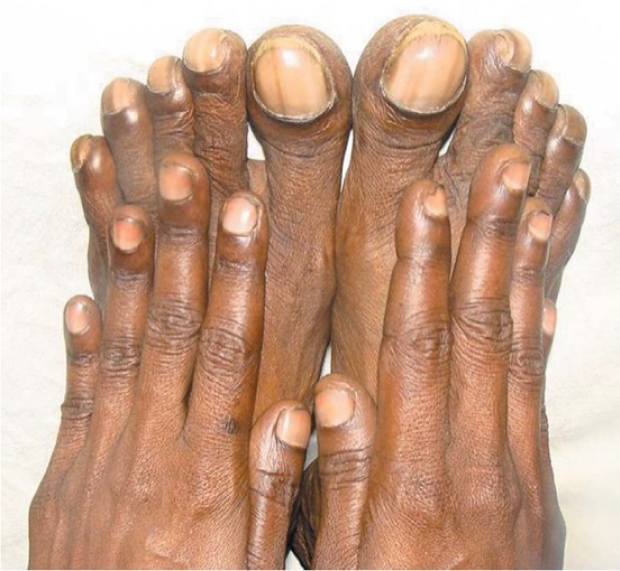
Figure 1. Obvious clubbing in patients toes. Note the relative severity in the toes compared to the hands. From (1) with permission.
The causes of clubbing are a favourite bedside question on rounds. They can be divided into:
Pulmonary (commonest – think neoplasm until proven otherwise).
- Bronchial carcinoma
- Mesothelioma
- Bronchiectasis
- Cystic fibrosis
- Interstitial fibrosis
Cardiac
- Cyanotic congential heart disease
- Infective endocarditis
- Atrial myxoma
Gastrointestinal
- Cirrhosis
- IBD
- Coeliac disease
Congenital
Which of these could cause the distribution in figure 1? If you need a further clue, here is another patient with the same condition.

Figure 2. The saturation in toes and fingers is different, despite the patient inspiring a constant oxygen concentration. Adapted from (2), with permission.
Answer Below…
These are pathognomonic physical signs. If a patient with a patent ductus arteriosus (PDA) develops Eisenmenger’s syndrome there will be arteriovenous mixing causing deoxygenated blood. Crucially this affects the lower limbs exclusively as the PDA connects pulmonary artery to aortic arch distal to the left subclavian artery. The exact mechanism by which hypoxaemia results in clubbing is not fully understood, but is thought to involve growth factors in vascular endothelium and platelets (See this article to learn more about the mechanism). Hence as the lower limbs experience more hypoxaemia, they develop more clubbing and cyanosis.
To demonstrate clubbing at the bedside, Shamroth’s window test is performed:
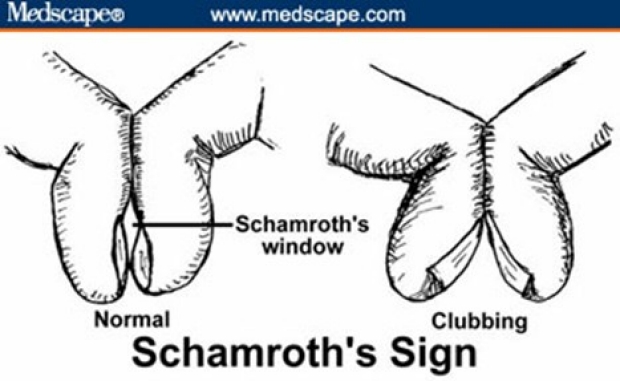
Figure 3. Shamroth’s window test showing obliteration of nail fold angle (no rhomboid visible) when clubbed nails are opposed.
For more examples of how important the hand is in physical diagnosis, refer to theStanford 25 page on the hand.
Take Home Message:
Clubbing and cyanosis that is worse in the lower limbs than upper limbs can only be explained by a patient with Eisemenger’s syndrome second to PDA.
Bonus question:
What cardiovascular examination findings would you expect in this patient?(Answer Below)
Cardiac auscultation revealed a left parasternal heave, a palpable second heart sound, single and loud S2 and a soft pansystolic murmur of triscupid regurgitation.
Clinical tips:
Once Eisemenger’s develops there is no flow murmur across PDA as the pressure in right and left heart are equal. This means a single loud S2, which may be palpable and signs of RV hypertrophy. Often there may be associated flow murmurs, but not the characteristic continuous machinery murmur of a PDA.
References:
1. Anoop T, George K. Differential Clubbing and Cyanosis. N Engl J Med 2011;364(7):666.
2. Moccetti F, Kaufmann B a., Tobler D. Differential clubbing and cyanosis: A pathognomonic finding in cardiology. Eur Heart J 2014;35(21):1410.