Examination of the Tongue
The tongue exam can reflect a number of underlying diagnoses such as infections, nutritional deficiencies, malignancy and even neurological dysfunction.
Technique of the Tongue Exam
On physical examination, there are several characteristics of the tongue that should be noted:
- Color
- Pink-red on dorsal and ventral surfaces. The ventral surface may have some visible vasculature.
- Texture
- Rough dorsal surface owing to papillae, which have three types. There should be no hairs, furrows, or ulceration.
- Size
- Should fit comfortably in mouth, tip against lower incisors. Sublingual glands should not be displaced.
In general, the examination of the tongue should occur in the following steps:
- Have the patient touch the tip of the tongue to the roof of their mouth and inspect the ventral surface.
- Have the patient protrude the tongue straight out and inspect for deviation, color, texture, and masses
- With gloved hands, hold the tongue with gauze in one hand while palpating the tongue between the thumb and index finger of the other, noting masses and areas of tenderness.
Clinical Findings in Tongue Pathology
Smooth Tongue
The most common cause of a smooth tongue is the use of dentures. Nutritional deficiencies include iron, folate and vitamin B12 deficiency. B12 deficiency will also make the tongue sore and beefy-red in color. Glossitis, by causing swelling of the tongue, may also cause the tongue to appear smooth. Among women, low-estrogen states may cause a “menopausal glossitis”.
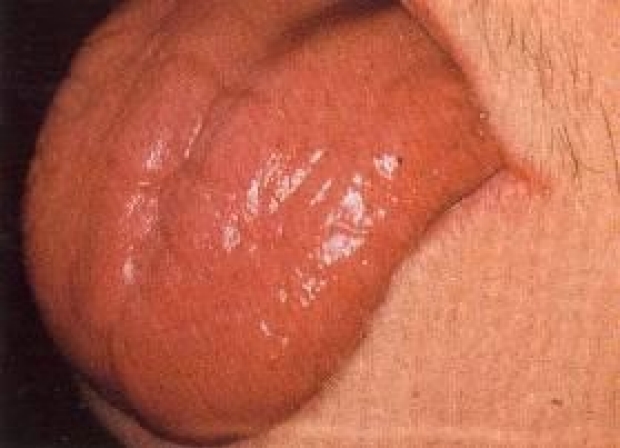
A classic smooth, beefy red tongue from vitamin B12 deficiency (Credit)
Geographic Tongue
Geographic tongue is a benign condition in which discolored, painless patches of the tongue appear and then reappear from atrophy, often in a different distribution. This is seen in 1-3% of the population.

Geographic Tongue (Credit)
{kind=link}
Hairy Tongue
White hairs along the sides of the tongue are the classic appearance of oral hairy leukoplakia, the result of EBV infection in HIV-positive individuals. A black hairy tongue in the setting of chronic administration of penicillins is often fungal overgrowth, particularly of aspergillus.

Oral Hairy Leukoplakia, in an HIV-positive individual. (Credit)
{kind=link}

A black, hairy tongue consistent with aspergillus overgrowth (Credit)
Furrowing
Transverse furrows across the tongue may be from a benign condition called scrotal tongue. Furrows that are longitudinal along the length of the tongue are the result of syphilis.
Ulcers
In inspecting ulcers, it is important to note their size, number, color, distribution, and whether or not they cause the patient any discomfort.
Aphthous ulcers, or aphthous stomatitis, are a painful form of ulcer that is frequently encountered. It appears in one of several patterns: minor, major, or herpetiform. Minor aphthous ulcers are usually 2-8mm in size and spontaneously heal within 14 days. Major aphthous ulcers are >1cm in size and may scar when they heal. Herpetiform ulcers are pin-point size, often multiple, and may coalesce to form a larger ulcer. All may result in odynophagia when they occur toward the posterior surface of the oropharynx.
Recurrent aphthous ulceration or stomatitis (RAU/RAS) occurs in some systemic illnesses. These include Crohn's Disease and Ulcerative Colitis, Behcet's Syndrome, pemphigus, herpes simplex, histoplasmosis, and reactive arthritis (Reiter's Syndrome). Other causes of RAU include drug reactions, Marshall Syndrome, and MAGIC (Mouth and Genital ulcers with Inflamed Cartilage) syndrome. The ulcers themselves may become infected, requiring treatment.
A single non-healing, erythematous, painful ulcer suggests lingual or oral cancer, particularly if the patient uses tobacco and/or alcohol. Patient history and risk factors are important to note.
Micro/Macroglossia
Microglossia may result from pseudobulbar palsy, damage to the upper motor neurons of the corticobulbar tracts that innervate the tongue. This presents with a small, stiff tongue. In newborns there may be an apparent microglossia resulting from a congenitally short lingual frenulum (ankyloglossia) commonly called a “tongue tie”.
Assessment of macroglossia should include palpation of the sublingual glands; these will be displaced in true macroglossia. Macroglossia may be congenitally present in individuals with acromegaly. New-onset macroglossia in an adult is pathognomonic for amyloidosis and should be treated as such until proven otherwise.
Fasciculations
Fasciculations of the tongue are indicative of lower motor neuron injury. These may present with dysarthria or dysphagia. New-onset fasciculations are concerning for amyotrophic lateral sclerosis.
Conditions in Tongue Disease
Lingual Cancer
Lingual cancer is the second most-common head and neck cancer, after that of the labia. Tobacco and alcohol use are both major risk-factors. The patient will often present with a painful mass in the tongue or a non-healing ulcer. There may be a history of leukoplakia, dysphagia, or dysarthria. Physical exam may reveal a tender lump in the tongue on palpation, however physical examination may not reveal anything if the mass is toward the posterior end of the tongue. A proper workup, which may include fine needle aspiration of the mass, is necessary for diagnosis.
Candidiasis
Oral candidiasis, or thrush, is the result of infection of the oropharynx by Candida albicans. This is most typically in patients with some form of immunocompromise, particularly HIV, diabetes, or chronic antibiotic use, which leads to fungal overgrowth. The patient presents with painless, white plaques on the tongue or oropharynx which are easily scraped off. Odynophagia concurrent with this suggests that the esophagus is also involved. Treatment includes any of a number of antifungals, including a nystatin gargle.
Key Learning Points
- Learn the technique of the inspection of the tongue
- Review of important clinical findings of the tongue
Related to the Tongue in Diagnosis
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam