Examination of the Hand (The Hand in Diagnosis)
The examination of the hand and nails can lead to a number of diagnoses. Some of these include liver disease (Terry's nails), kidney disease (Lindsay's nails), lung disease (nail clubbing), endocarditis and many others.
Introduction to the Hand Exam
![]() Consider beginning all physical examinations by reaching for the patient's right hand with both of yours. Inspect it and then move to the radial pulse. This is a nice way to ease into the examination; you are beginning with the equivalent of a handshake.
Consider beginning all physical examinations by reaching for the patient's right hand with both of yours. Inspect it and then move to the radial pulse. This is a nice way to ease into the examination; you are beginning with the equivalent of a handshake.
Handshake:
- Moist and warm hands (think nervousness, thyrotoxicosis, look for tremor, eye signs).
- Inability to let go your of hand (think myotonia, not to be confused with the grasp reflex in frontal lobe disease. Look for other signs of myotonic dystrophy: hatchet face, cataracts, baldness, myopathic facies).
Mechanical Dysfunction of the Hand
Misc. Hand Findings
Nails
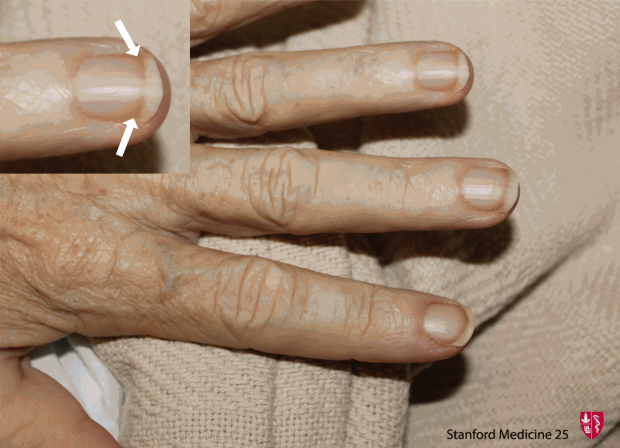
Terry's Nails
Proximal paleness extending halfway up the nail, often eliminating the lunula. Darker distal band. Seen in states of stress (e.g. advanced age, liver disease/cirrhosis, CHF, DM2). (Image Credit)


Muehrcke's Lines (Leukonychia striata)
Narrow while transverse lines (Not depressed, compared to Beau's lines). Usually 2 or more lines on one nail. Seen in states of decreased protein synthesis or increase protein loss such as with hypoalbunemia (usually less than < 2.2 g/dL), certain chemotherapy and nephrotic syndrome. (Image Credit)

Mees' Lines
Transverse while lines (usually one per nail, no depressions) that often can will disappear if pressure is placed over the line. It is strongly associated with arsenic poisoning, thallium poisoning and to a lesser extent other heavy metal poisoning. (Image Credit)


Splinter Hemorrhages
Nonspecific finding associated with trauma most commonly but also seen in subacute bacterial endocarditis and scleroderma. (Image Credit)

Nail Pitting
Non-specific sign for psoriasis (additional signs include onycholysis, thickening, and 'oilspot' lesions which are yellow patches on the nail). (Image Credit)

Quitter's Nail
Nicotine stained distally, but not proximally with clear line of demarcation. See also our article in Chest and NEJM clinical image. May also appear when pt switches to "lower tar" tobacco.

.gif)
Finger nails grow at a rate of about 0.8-1.0 mm per week. Using this, you can approximate when the clinical scenario causing the nail finding occurred. For example, approximating when someone has stopped smoking who has quitter's nails.
.gif)
Paronychia
Inflammation of the nail folds - red, swollen, often tender. Frequent immersion in water a risk factor for chronic paronychia. (Image Credit)


Important causes of clubbing in the adult:
- Lungs
- Lung Cancer (clubbing is in general an ominous sign for this, and remember "beware of the yellow clubbed digit". (Yellow from nicotine, and clubbed from cancer).
- Pus in the lung (bronchiectasis as in CF, but also lung abscess and empyema)
- Pulmonary Fibrosis
- COPD IS NOT A CAUSE OF CLUBBING (if you seen clubbing in a COPD patient, think lung cancer)
- Heart
- R to L shunts
- Endocarditis
- Pericarditis
- There are other causes of clubbing, outside the heart and lungs, but these are the important ones.
- If a patient has painful wrists, painful ankles and comes to see you and you miss that they also have clubbing, you will go down the wrong path looking for RA etc, when what they have is Hypertrophic Pulmonary Osteoarthropathy. The causes of HPOA are the same as those of clubbing.
Pseudoclubbing: distinguished from clubbing by the preservation of the nail-fold angle and bony erosion of the terminal phalanges on radiography. Pseudoclubbing is also more likely to be asymmetric.
Mechanical Dysfunction of the Hand
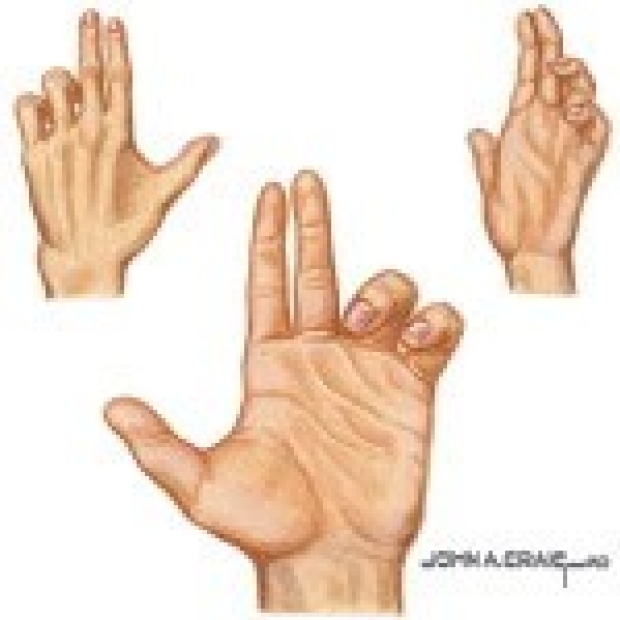
Pope's Hand (Hand of Benediction)
The pope's hand is seen with median nerve dysfunction when asking the patient to make a fist due to inability to flex 1st & 2nd fingers at PIP. The median nerve controls the 1st & 2nd lumbricals, three thenar muscles (abductor pollicis brevis, flexor pollicis brevis, and via a distal branch the opponens pollicis).Additionally theremay be thenar atrophy. (Image Credit)
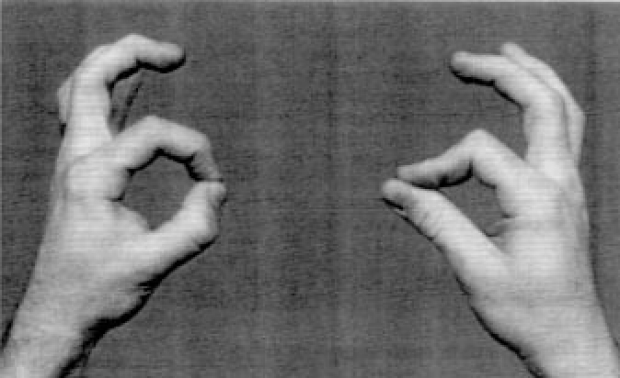
Ask patient to use both hands to make and "Okay" sign by forming a circle with thumb and index finger. Median nerve palsy may make one hand produce a pinched circle (right hand in image). (Image Credit)
Ape Hand
Distal median nerve dysfunction: Inability to oppose thumb from distal median nerve dysfunction.
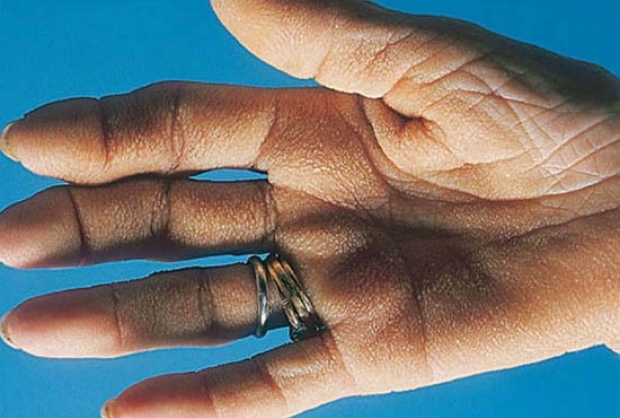
Claw Hand
The image below is a simulated claw hand. Note that due to ulnar damage, the 3rd & 4th lumbricals are unable to extend the PIP & DIP joints at the 4th & 5th digits.
The ulnar nerve controls the 3rd & 4th lumbricals, the three hypothenar muscles, the dorsal & palmar interossei, the palmaris brevis and the adductor pollicis. Ulnar nerve damage may also cause hypothenar atrophy.

Froment's Sign
Ask patient to hold a piece of paper between thumb and index finger. If the examiner can pull paper away (a positive Froment's sign), it suggests that an ulnar palsy has weakened the thumbs strength of opposition.
Radial nerve damage
No intrinsic muscles but important wrist extensors. Radial nerve damage commonly causes wrist drop.
.jpg)
Misc. Hand Findings
Herpetic Whitlow
Occupational hazard for respiratory therapists and house staff who work around oral secretions. (Image Credit)


Hypermobility of hand joints
Ehlers Danlos, many types. Syndrome may include skin hyperextensible, fragile, "cigarette paper burn" scars, spontaneous rupture of eye, arteries, intestine, hip dislocations, Marfanoid habitus, kyphoscoliosis, prominent hernia, mitral valve prolapse, coronary dissection.
Short extremities and polydactyly
Ellis Van Creveld Syndrom - dwarfism, short extremities and polydactyly, dysplastic teeth and nails, multiple frenula binding the upper lip to the alveolar ridge, ASD or a single atrium.
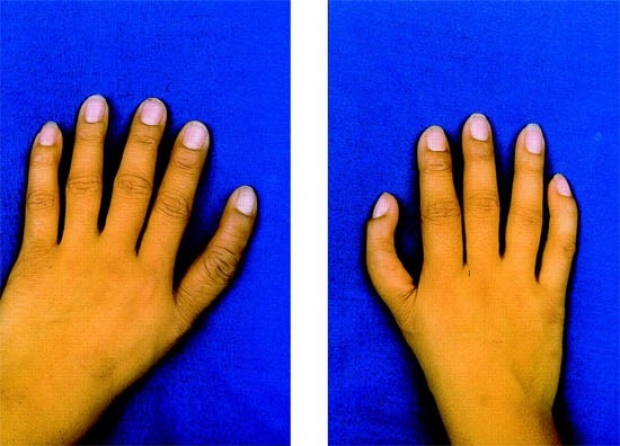
Arachnodactyly (Achromachia)
- Long "spider-like" digits, thumb can often extend beyond palm. Characteristic of Marfan's Syndrome - tall stature, thoracic deformity, joint laxity, ectopia lentis and myopia, aortic dilation and dissection, mitral valve prolapse, autosomal dominant, spontaneous pneumothorax, chordae tendineae rupture.
Tripe Hand
Thickened, velvety texture of hand. Often sign of visceral malignancy. See also NEMJ "Velvet Palms" in Images in Clinical Medicine. (Image Credit)

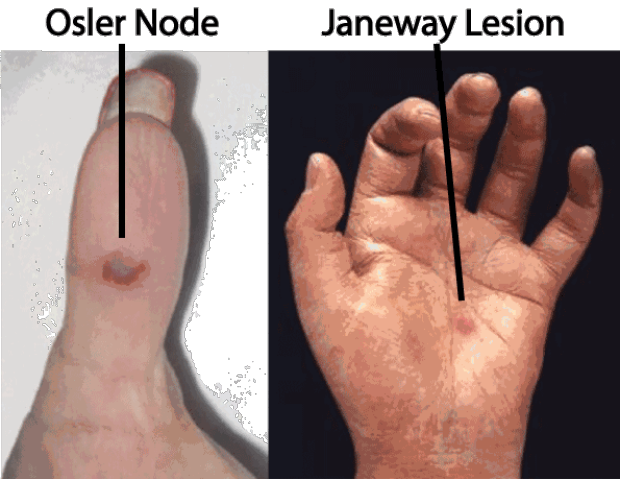
Janeway Lesions vs. Osler Nodes
Both found in bacterial endocarditis.
- Osler Nodes:
- Painful, palpable red lesions usually on fingers/toes. They are caused by immune complexes. (Image Credit)
- Janeway Lesions
- Non-painful, macular lesions, usually on palms/soles. They are caused by septic emboli, more common in Staph aureus endocarditis. (Image Credit)
(See Splinter Hemorrhages and Roth Spots)
Key Learning Points
- Learn nail pathology
- Learn mechanical dysfunction of the hand
- Review misc. hand findings
Related to The Hand in Diagnosis
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam