Thyroid Exam
The thyroid exam is important as it’s often the first step towards diagnosing thyroid diseases such as Grave’s disease, Hashimoto’s thyroiditis and multinodular goiters. Both inspection and palpation are important aspects of the thyroid exam.
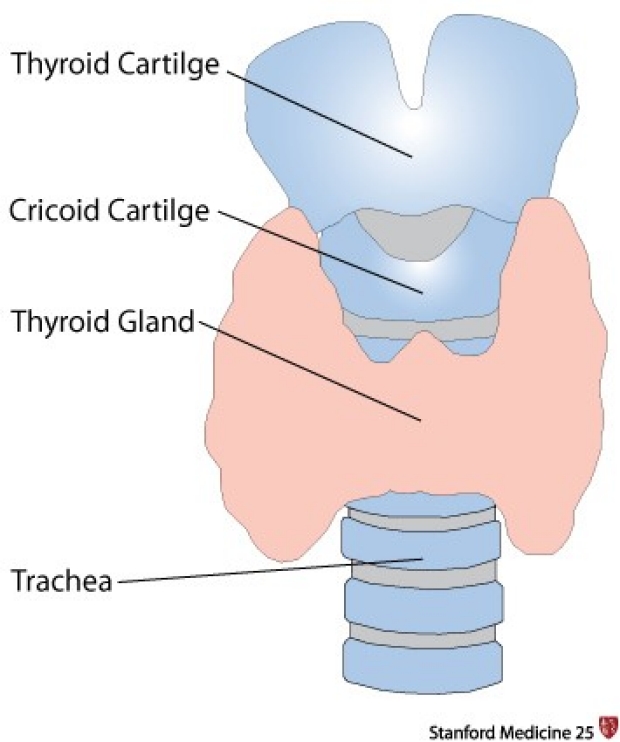
Anatomy of the Thyroid
Too often when people are feeling for the thyroid, their fingers are nowhere near the thyroid gland. The thyroid cartilage, despite its name, is not where the gland is situated.
Palpation of the Thyroid
Now that you know the anatomy, you will need to identify the landmarks listed below.
Do this on yourself or someone:
- Put your finger on tip of your chin (mentalis).
- Slide finger down the midline and the first hard structure you hit is the top of the thyroid cartilage. (Surprisingly, one does not feel the hyoid bone in the midline, although sometimes its lateral end is misidentified as a hard lymph node).
- Run your finger down the prow or the free edge of the thyroid cartilage (Adam's apple).
- The next thing you hit is the cricoid cartilage (and see if you can get your fingernail in between the thyroid and cricoid cartilage–that is the cricothyroid membrane which is where trans-tracheal aspirations for pneumonia can be performed).
- Below the cricoid ring are the first two rings of the trachea, and the ISTHMUS of the thyroid overlies those two rings.
- Ask patient to flex neck slightly forward and relax.
- Go through the landmarks as above.
- Place first two digits of both hands just below cricoid cartilage so that left and right fingers meet on the patient’s midline. Place thumbs posterior to patient’s neck and flatten all fingers against the neck.
- Use finger pads, not tips, to palpate.
- Identify the isthmus.
- Gently draw fingers laterally 1-2cm.
- Gently palpate lateral lobes.
- NOW ask patient to swallow (give them a glass of water if possible).
- Assess for asymmetrical elevation of lobes (suggests nodularity).
- When you are done with above, move to next phase, which is displacing the soft tissues on one side to the midline while assessing for size with the other hand. Repeat in opposite direction.
Consult the Expert
Dr. Neil Gesundheit
Dr. Neil Gesundheit is an endocrinologist and an Associate Dean for Advising for the School of Medicine at Stanford. He has published extensively on both medical student education and clinical endocrinology.
Clinical Pearl
Most North American patients have small thyroids (15-20 gm in weight) and thus closer to the midline. For such patients, if palpating from behind, to place index and middle fingers only 2-3cm apart (off the midline). If fingers are too lateral, they might not detect the contours of the average North American thyroid.
Findings in Thyroid Disease
Thyroid Enlargement
- Diffuse Enlargement: isthmus and lateral lobes, no nodules. Grave’s disease, Hashimoto’s thyroiditis, endemic goiter
- Single node: Cyst, benign tumor, false positive (only one nodule of multinodular goiter detected). Elevates index of suspicion for malignancy.
- Assess for risk factors: radiation exposure, hardness, rapid growth, fixation to surrounding tissue, cervical LAD, male, others.
- Multinodular Goiter (iodine deficiency)
Soft in Graves Disease and may have bruit.
Firm in Hashimoto’s thyroiditis, malignancy, & benign and malignant nodules.
Tender in thyroiditis.
Systolic or continuous bruit may be heard over lateral lobes in hyperthyroidism.
Key Learning Points
- Learn the anatomy of the thyroid gland
- Learn the correct technique to palpate the thyroid gland
- Describe the findings seen in the thyroid exam
Related to Thyroid Exam
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam