Carpal Tunnel Exam
Carpal Tunnel Syndrome is the most common nerve entrapment syndrome, affecting approximately 3.8% of the general population.
Introduction to the Exam for Carpal Tunnel
Carpal Tunnel Syndrome is the most common nerve entrapment syndrome, affecting approximately 3.8% of the general population [1]. The pathophysiology involves increased pressure on the median nerve as it traverses through the carpal tunnel leading to impaired blood flow, inflammation, and ischemic injury of the nerve [2]. The median nerve has both motor and sensory functions, which can be affected in carpal tunnel syndrome [1-3].
Early in the disease course, clinical features revolve around sensory deficits of the median nerve, with associated paresthesia, pain, and/or numbness in the palmar surface of the thumb, index, middle, and radial half of the ring finger [3]. Rarely, patients may also report pain radiating proximally from the wrist towards the elbow [2]. Sensory symptoms tend to occur with repetitive hand movements, sustained hand/ wrist postures, and often worsen at night [2]. In later stages, patients may develop motor deficits of the median nerve with associated weakness of the thenar muscles leading to impaired pinch and grip of the hand [3].
Inspection
The clinical exam for carpal tunnel syndrome should begin with inspection of the hands for signs of osteoarthritis, symmetry, and muscle atrophy. Late stages of carpal tunnel syndrome can lead to profound thenar atrophy, as the abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis are innervated by the median nerve. Thenar atrophy can be seen visually and/ or palpated in comparison with unaffected hand.

Thenar atrophy.
Motor Exam
The median nerve supplies motor innervation to the abductor pollicis brevis, flexor pollicis, brevis, and opponens pollicis (together forming the thenar eminence), as well as the lumbricals of the first and 2nd digits. However, the flexor pollicis brevis, opponens pollicis, and the lumbricals have varying degrees of overlapping innervation from other nerves, making the abductor pollicis brevis the best measure of median nerve motor dysfunction. This can be achieved by placing the patient’s hand palm side up on the exam table and putting the thumb into flexion. Instruct the patient to resist any movement while using your middle finger to try to extend the thumb flat against the table. Your index finger can simultaneously palpate the thenar eminence, assessing for degree of muscle contraction during patient’s resistance of movement. Grade the degree patient can resist movement using MRC grading system of 0-5 for strength.

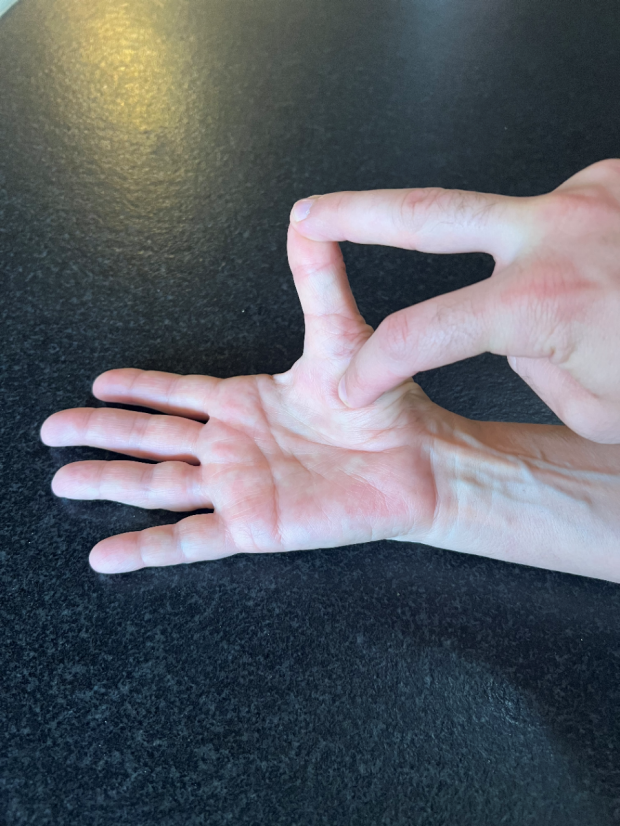
Strength Assessment of Abductor Pollicis Brevis: Place patient’s thumb into abduction, instruct patient to resist movement while pressing thumb into adduction and palpating thenar eminence to assess for strength of abductor pollicis brevis (solely innervated by the median nerve).
Sensory Exam
Assess the sensory distribution of the median nerve using a rating system of 0 to 10, with 0 being no feeling at all and 10 being normal sensation. First, have patient close their eyes. Then, pick a location where patient has no complaints of sensory disturbances (like the forearm) and lightly stroke the area with your finger, instructing the patient that if this sensation is 10 out of 10, please tell me from 0 (being no sensation at all) and 10 (being this sensation) how each of the following areas feel. Proceed to lightly stroke areas of the hand innervated by the median nerve, noting regions of decreased or abnormal sensations.
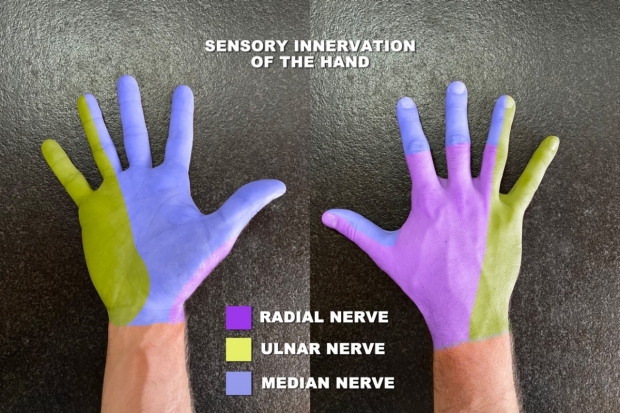
It can be useful to also comparatively assess sensation between areas innervated by the ulnar nerve and median nerve (for example: compare sensation of palmar 5th digit with palmar thumb. If patient symptoms are unilateral, it can also be useful to compare sensation of the same anatomic location on each side. Importantly, the palmar cutaneous branch of the median nerve exits proximal to the carpal tunnel and supplies sensory innervation to the thenar eminence, which should therefore be spared of numbness even in severe cases of carpal tunnel syndrome [2].
Provocative Maneuvers
There are multiple provocative maneuvers designed to induce symptoms of paresthesia that can aid in the clinical evaluation of carpal tunnel syndrome.
Phalen’s Test
Sensitivity: 68% [6]
Specificity: 73% [6]
Phalen’s Test was first described in 1957 and is one of the most widely used clinical tests to evaluate for carpal tunnel syndrome [5]. There are many versions of the Phalen’s test, but they all involve prolonged wrist flexion for up to one minute to increase pressure in the carpal tunnel.

Modified Phalen’s Test: Patient places wrist dorsum together for one minute. Positive result occurs if patient develops pain, paresthesia, or numbness in the median nerve distribution [6]
Reverse Phalen’s Test (AKA Wormser’s Test)
Sensitivity: 57% [6]
Specificity: 78% [6]
The reverse Phalen’s test or Wormser’s test is performed by placing the palms together to cause bilateral wrist extension, which also increases pressure in the carpal tunnel [6].

Modified Reverse Phalen’s Test (AKA Wormser’s Test): Patient places palms together, increasing pressure in the carpal tunnel. Positive result occurs if patient develops paresthesia in median nerve distribution [6].
Tinel’s Test
Sensitivity: 50% [6]
Specificity: 77% [6]
Tinel’s test involves the examiner tapping over the volar carpal ligament, along the median nerve at the carpal tunnel for up to 60 seconds [4]. A positive test result (AKA Tinel’s Sign) occurs if the patient reports tingling or electric shocks along the distribution of the median nerve [4, 6]. Importantly, the sensitivity of Tinel’s Test can be increased by using a Queen’s square reflex hammer instead of fingers to tap over the carpal tunnel [6].


Tinel’s Test: Examiner repeatedly taps over the volar carpal ligament for up to 60 seconds. The test is considered positive if patient reports tingling or electric shocks in distribution of the median nerve [4, 6].
Carpal Compression Test (Durkan’s)
Sensitivity: 64% [6]
Specificity: 83% [6]
The Carpal Compression Test or Durkan’s Test is performed by holding the patients wrist in slight flexion and directly compressing the median nerve by applying pressure to the proximal wrist crease for 30 seconds. A positive result occurs if patient develops pain, paresthesia, or numbness in median nerve distribution.

Proper Technique for Carpal Compression Test (Durkan’s): Note examiner should apply pressure directly over the proximal wrist crease for 30 seconds. Test is considered positive if patient develops pain, paresthesia, or numbness in median nerve distribution.
Hand Elevation Test
Sensitivity: 75.5% [7]
Specificity: 98.5% [7]
The hand elevation test is the most specific of the provocative maneuvers for carpal tunnel syndrome. The test was developed in 1999 by Duck-Sun Ahn after he observed that patients with carpal tunnel syndrome had paresthesias when holding their hands against gravity (like on subway railings and straps on buses) [7]. The resulting hand elevation test was designed by having patients raise their hands above their head using their own strength for up to two minutes, with the elbows and shoulder in loose flexion [7]. The test is considered positive if paresthesia, pain, or numbness develops within two minutes [7].

Hand Elevation Test: Patient holds hands over head with elbows and shoulders in loose flexion for up to two minutes. Test is considered positive if paresthesia, pain, or numbness develops [7].
Sources
1.) Atroshi, Gummesson, Johnsson, Ornstein, Ranstam, and Rosén I. Prevalence of Carpal Tunnel Syndrome in a General Population. JAMA. 1999;282(2):153–158. doi:10.1001/jama.282.2.153
2.) Ibrahim I, Khan WS, Goddard N, Smitham P. Carpal tunnel syndrome: a review of the recent literature. Open Orthop J. 2012;6:69-76. doi: 10.2174/1874325001206010069. Epub 2012 Feb 23. PMID: 22470412; PMCID: PMC3314870.
3.) Aroori, Somaiah, and Roy A J Spence. “Carpal tunnel syndrome.” The Ulster medical journal vol. 77,1 (2008): 6-17.
4.) Hoppenfeld, Stanley, and Richard Hutton. Physical Examination of the Spine and Extremities. , 1976. Print.
5.) PHALEN, GEORGE, . "The Carpal-Tunnel Syndrome". The Journal of Bone & Joint Surgery, vol. 48, no. 2, March 1966, pp. 211-228.
6.) MacDermid, Joy C, and Jean Wessel. “Clinical diagnosis of carpal tunnel syndrome: a systematic review.” Journal of hand therapy : official journal of the American Society of Hand Therapists vol. 17,2 (2004): 309-19. doi:10.1197/j.jht.2004.02.015
7.) Ahn, Duck-Sun, . "Hand Elevation: A New Test for Carpal Tunnel Syndrome". Annals of Plastic Surgery, vol. 46, no. 2, February 2001, pp. 120-124.
Key Learning Points
- Learn inspection
- Learn the motor exam
- Review provocative maneuvers
Related to The Carpal Tunnel Exam
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam