Precordial Movements in the Cardiac Exam
As the heart contracts, movements can be palpated and often visualized over the chest. The location and character of these precordial movements correlate with abnormalities of the heart, such as in hypertrophic heart disease.
Introduction to Precordial Cardiac Exam
Both the observation and palpation of the point of maximal impulse (PMI) of heart is part of a complete cardiac exam. These exam findings can yield important information about the heart such as a laterally displaced PMI in an enlarged heart.
The Apex Cardiogram
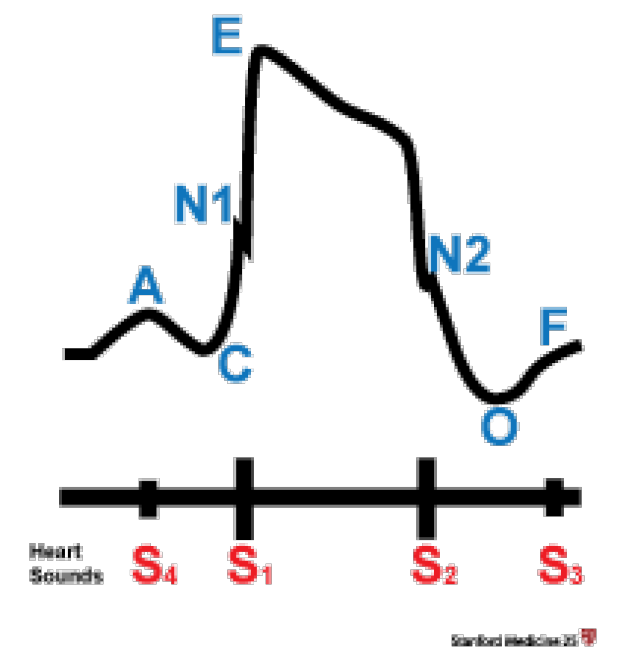
Shown is the curve created by the PMI measured by an apex-cardiogram. Although now used infrequently, this device can be used to help diagnose ventricular abnormalities and is shown here to better understand the normal PMI.
(A = left ventricular filling; C = systolic wave; E = systolic peak; O = start of rapid filling (mitral valve open); F = start of slow filling [diastasis].)
Observation of the Point of Maximal Impulse
Observation of the PMI can be challenging. It is best seen in thin-chested patients.
Prior to observation, have your subject lay flat, you should observe the pulsations from the PMI from the side of the subject.
Exam findings
- Normal
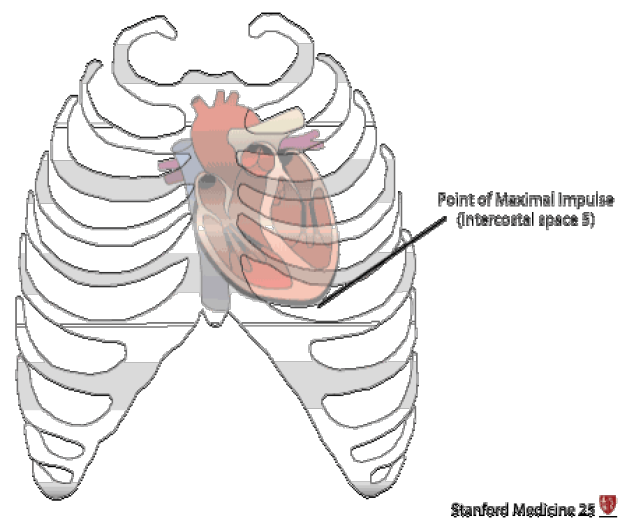
- The normal PMI is usually located inside the mid clavicular point at intercostal space 5 (see figure below)
- Observe a single outward impulse, representing the systolic contraction of the left ventricle ("E" wave in figure above)
- Abnormal
- Double impulse: visible over the apical region seen in hypertrophic cardiomyopathy (this is caused by a second impulse after the first one from filling of the enlarged ventricle during diastole, 'a' wave in figure above)
- Lateral displacement of the PMI (to left): usually seen in an enlarged heart (also seen in right large pleural effusion, right tension pneumothorax and left-sided pulmonary fibrosis)
- Epigastric & subxiphoid movements: usually seen in with right ventricular hypertrophy, right ventricular dilation or an abdominal aortic aneurysm
- Can also be normally seen with emphysema, children or a scaphoid abdomen and the very thin
- Right 2nd intercostal pulsation: may indicate an aneurysm of ascending aorta
- Left 2nd (or 3rd) intercostal pulsation: less common, can be seen with a dilated pulmonary artery
- Retraction of chest wall: seen in biventricular hypertrophy or constrictive pericarditis
Palpation the Precordial Cardiac Exam
Introduction to palpation
- When palpating for the PMI, your finger pads are more sensitive than finger tips.
- Along with palpating for near the apex, you should also palpate both lower parasternal, pulmonary, aortic, suprasternal and epigastric regions for a complete exam.
- Somtimes, it will be difficult to palpate the PMI in certain conditions such as extreme tachycardia or shock.
- Checklist of questions when examining PMI:
- Position:
- Normally 5th intercostal space near the mid-clavicular line. Is it displaced?
- Area?
- Size of dime versus quarter
- Amplitude?
- Normally 'brisk' or 'tapping.'
- Is it 'heaving' (i.e. is the ventricle doing 'pressure' work)?
- Is it 'hyperdynamic' (i.e. is the ventricle doing 'volume' work)?
- What is its character ?
- Is it single (normal) or a double impulse (e.g. hypertrophic cardiomyopathy)
- Is there a parasternal heave? (right ventricular hypertrophy)
- Pulsations in other areas?
- Right 2nd intercostal pulsations? (aneurysm of ascending aorta)
- Left 2nd intercostal pulsations? (dilated pulmonary artery)
- Is there a thrill?
- Seen with loud (grade > 4/6) murmurs
- Position:
Exam findings
- Normal
- The normal PMI is usually located near the mid-clavicular point at intercostal space 5
- A normal, non-sustained tapping should be felt, that is no larger than 2-3cm in diameter
- Should be a single impulse per cardiac cycle
- There should be no impulses felt at other locations other than the apical region
- Abnormal
- Forceful & Hyperdynamic: this is appreciated as a fast impulse with a large amplitude that terminates quickly; it does not extend through systole
- Seen with states of increased "volume" work:
- Exercise
- Hypermetabolic states (anemia, hyperthyroid, high-cardiac output)
- Mitral regurgitation/aortic regurgitation/ventricular septal defect
- Forceful & Sustained: this outward movement is sustained throughout systole (would be a plateau shape on apex cardiogram) -- indicative of a ventricle doing "pressure" work
- Seen with left ventricular hypertrophy or states of outflow obstruction making the heart pump harder (e.g. high blood pressure)
- A sustained impulse can also be seen in cardiac heart failure with a reduced ejection fraction
- Seen with left ventricular hypertrophy or states of outflow obstruction making the heart pump harder (e.g. high blood pressure)
- Double impulse: in this the second impulse is from the exaggerated 'a' wave ('a' wave in figure above) that is normally not palpable and represents left ventricular filling during diastole. However in states of elevated end-diastolic pressure, the 'a' wave will increase and be palpable causing the "second" impulse.
- These states include:
- left ventricular hypertrophy (concentric hypertrophy as in aortic stenosis, hypertension, hypertrophic cardiomyopathy)
- myocardial disease/cardiomyopathy
- non-compliant heart in any form of ischemia
- Left lower parasternal palpation (heave)
- Located at the left parasternal intercostal spaces 3 & 4
- May be normal in children or small/thin adults but if present throughout systole, then likely pathologic and suggestive of right ventricular hypertrophy
- Other precordial pulsations
- Right 2nd intercostal pulsation: may indicate an aneurysm of ascending aorta
- Left 2nd (or 3rd) intercostal pulsation: less common, can be seen with a dilated pulmonary artery
- Forceful & Hyperdynamic: this is appreciated as a fast impulse with a large amplitude that terminates quickly; it does not extend through systole
Precordial Movements of the Cardiac Exam: The Double Impulse
.gif)
The point of maximal impulse (PMI) is simply that... the point where there is a maximal impulse against the chest that can be felt. Most often, this is from the apex or tip of the heart: also referred to as the apical impulse. However, in certain conditions, the apex of the heart does not cause the PMI. For example, in a severe right ventricular dilation, a left lower parasternal heave many be the largest impulse felt. This is in part from the right ventricular rubbing against the anterior chest wall at the left parasternal region and also from the enlarged right ventricle causing posterior displacement of the apex.
.gif)
Key Learning Points
- Learn the proper technique observing the precordial movement
- Learn the proper technique palpating the precordial movement
Related to Precordial Movements
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam