Pulmonary Exam: Percussion & Inspection
The pulmonary exam is one of the most important and often practiced exam by clinicians. While auscultation is most commonly practiced, both percussion and inspection are equally valuable techniques that can diagnose a number of lung abnormalities such as pleural effusions, emphysema, pneumonia and many others.
Introduction to the Pulmonary Exam
Though taught extensively in early medical training the pulmonary exam is often neglected apart from auscultation.
Percussion During the Pulmonary Exam
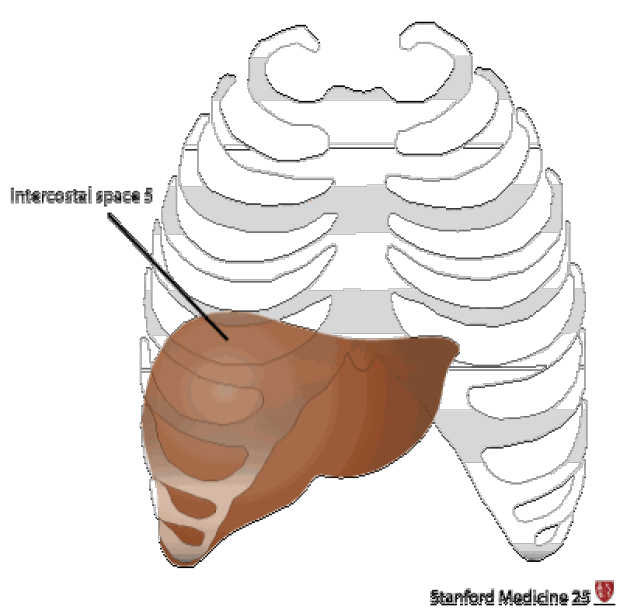
The "5-7-9 rule"
- The upper border of liver dullness is defined by:
- 5th intercostal space in the midclavicular line
- 7th intercostal space in the midaxillary line
- 9th intercostal space in the scapular line
- Note: 9th intercostal space is located approximately at the inferior border of the scapula
- Hyperresonance that continues below these boundaries can be suggestive of hyperinflation (e.g. emphysema)
Cardiac dullness
Be able to outline the area of "absolute" cardiac dullness— a fist sized area just to the left of the sternum. If it is not there it suggests emphysema.
Traube's space
- Surface markings:
- Superiorly: Left 6th rib
- Inferiorly: Left costal margin
- Laterally: Anterior axillary line
- Usually, traube's space is hyperresonant due to the location of the gastric bubble, however, loss of this hypersonance can be seen in following conditions:
- Left pleural effusion (however NOT in left lower lobe pneumonia without effusion as it is the effusion that falls into the costophrenic recess that is above the gastric bubble)
- Splenomegally (less reliable compared to Castell’s Sign)
- Very full colon
- Recently eaten (i.e. stomach is full)
Tidal Percussion
- Percuss down the back until the normal hyperresonance of the lungs becomes dull over the diaphragm. Then simply have the patient breath in and out deeply while continuing to percuss. The sound should wax and wane.
- Loss of tidal percussion:
- Pleural effusion
- Hyperinflation such as emphysema from a maximally contracted diaphragm
Major and Minor Fissures of the Lung
- The major fissure can be located by drawing a line from the T2 spinous process to where the 6th rib meets the sternum. The minor fissure can be approximated by drawing a horizontal line from the 4th rib attachment of the sternum to the major fissure.
- Easier method: Simply ask the patient to put their hands over their head. The scapula will rotate externally and its medial border will outline the major fissure (see figure below).


Historical Perspective of the Pulmonary Exam
Percussion was first described by Dr. Josef Leopold Auenbrugger, an Austrian physician who first observed his father tapping on wine barrels in the cellar of his hotel to determine how much wine was left. The son applied this technique to patients when he became a physician. He is credited with bringing the technique of percussion to the field of medicine. Much of his work occurred around 1760 where he described that by percussing the thorax he could accurately predict the contents of what was inside, as confirmed with post-mortum studies he conducted.
Inspection During the Pulmonary Exam
Signs of COPD
- Inspiratory descent of trachea.
- Use of accessory muscles.
- Pursed lips on exhalation (provides a small amount of PEEP).
- Increased AP diameter (barrel chest).
- Normal in infancy and increased with aging.
- Prominent angle of Louis (or sternal angle).
- Flaring of the lower costal margins.
- Dahl Sign: Above the knee, patches of hyperpigmentation or bruising caused by constant 'tenting' position of hands or elbows.
- Hoover's sign: briefly, during inspiration a paradoxical medial movement of the chest.
- The "subcostal angle" is the angle between the xiphoid process and the right or let costal margin. Normally, during inhalation the chest expands laterally, increasing this angle. When the diaphragms are flattened (as in COPD), inhalation paradoxically causes the angle to decrease.
- Harrison's sulcus: a horizontal grove where the diaphragm attaches to the ribs; associated with chronic asthma, COPD, & Rickets.
REMEMBER : "The side that moves less, is the side of disease!"
Look for signs of volume loss (or gain) on the side that moves less(hollow supraclavicular fossae, intercostal spaces prominent, shoulder droopy, scapula outline more prominent).
Consult the Expert

Dr. Peadar Noone
Dr. Peadar Noone trained in Galway, Dublin, Boston, the UK and Chapel Hill, where he is now Associate Professor of Medicine and Medical Director of the Lung Transplant Program at the University of North Carolina, Chapel Hill.
Clinical Pearl
Insert (in a normal individual) three fingers vertically in the space under the cricoid cartilage, and above the sternal notch. As the person breathes in, the space may reduce to two fingers at most (i.e. the fingers get "squeezed" as the sternum rises with inspiration). In a patient with severe hyperinflation, the crico-sternal distance is much shorter (because the sternum is elevated), maybe 1-2 fingers at most. With inspiration one's fingers get "squeezed" out as the already "high" sternum rises up to the level of the cricoid, thus, in many cases, obliterating the crico-sternal distance altogether. Some clinicians label this sign "tracheal shortening" but strictly speaking, the actual tracheal length does not get shorter. Classically this is seen with severe emphysema / hyperinflation, or severe air trapping. Often accompanied by reduced hepatic and cardiac dullness on percussion, a widened / flared costal angle, and Hoover's sign.
Other Findings in the Chest
- Pectus Excavatum (Funnel Chest): depression of sternum; in severe cases may compress heart and great vessels.
- Pectus Carinatum (Pigeon chest): anterior displacement of sternum, usually benign.
- Flail Chest: secondary to multiple rib fractures, depression of diaphragm causes injured area to cave inward producing a "paradoxical thoracic movement" in breathing.
Key Learning Points
- Percussion of the lung exam
- Inspection of the lung exam
Related to Pulmonary Exam: Percussion & Inspection
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam