Tarsal Tunnel Exam
Tarsal Tunnel Syndrome (TTS) is a mononeuropathy caused by compression of the posterior tibial nerve or its branches in the foot/ankle.
Introduction to the Exam for Tarsal Tunnel
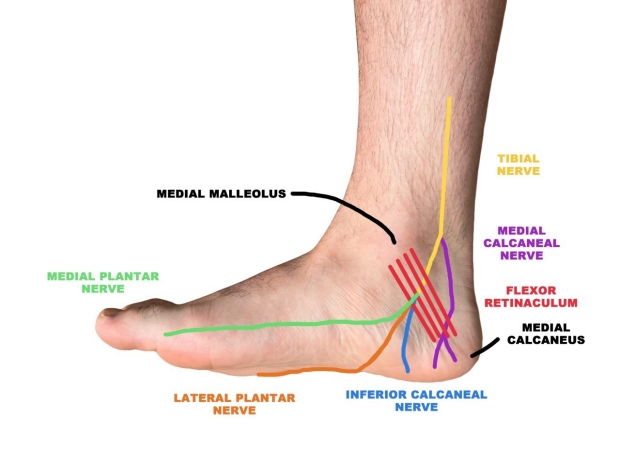
Tarsal Tunnel Syndrome (TTS) is a mononeuropathy caused by compression of the posterior tibial nerve or its branches in the foot/ankle [1]. TTS is analogous to Carpal Tunnel Syndrome, but occurs much more rarely, and usually as a result of trauma (fracture or sprain of the ankle), arthritis, or space-occupying lesions [2]. The tarsal tunnel runs deep to the flexor retinaculum of the ankle (connective tissue that connects medial malleolus with medial calcaneus), just posterior to the medial malleolus [2].
The clinical features of TTS are primarily paresthesia (tingling or pins and needles), hyperesthesia (increased sensitivity), and pain ranging from the posterior medial malleolar area to the sole, heel, and toes [2]. The symptoms may also radiate proximally up the calf, and typically worsen at night or with prolonged activity/ standing [2].
Anatomy
The tibial nerve arises from L4-S3 ventral divisions as part of the sciatic nerve and provides motor innervation to the posterior compartment of the leg, as well as sensory innervation to the foot and heel. The posterior tibial nerve gives off a branch to the medial calcaneus called the medial calcaneal nerve about 10cm proximal to the tarsal tunnel, supplying sensory innervation to the medial heel. Within the tarsal tunnel, the tibial nerve branches to form the lateral plantar nerve, medial plantar nerve, and the inferior calcaneal nerve, all of which can be compressed in tarsal tunnel syndrome. Notably, the inferior calcaneal nerve can be compressed in tarsal tunnel syndrome, leading to paresthesia and pain in the inferior heel, which often presents similarly to plantar fasciitis, a much more common condition.
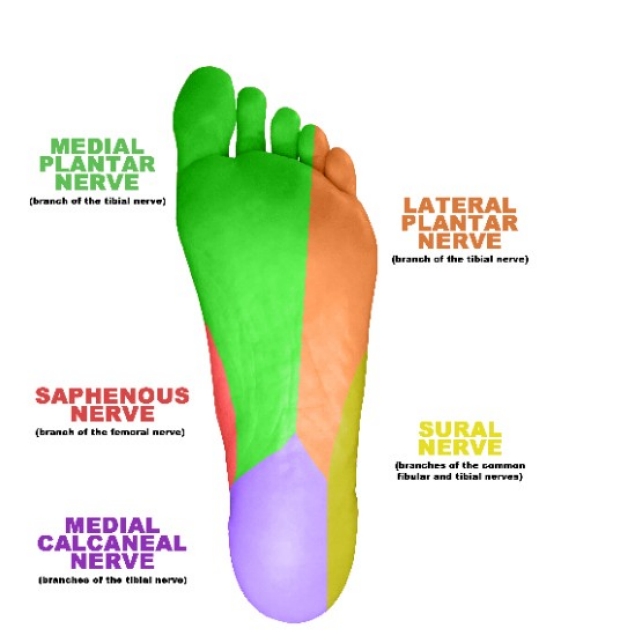
Sensory Innervation of the Foot
Inspection and Palpation
The exam for tarsal tunnel syndrome begins with inspection of the medial malleolus and medial foot, looking for obvious deformities, masses, and overlying skin changes. Severe tarsal tunnel syndrome can cause atrophy of the intrinsic muscles of the foot, which are only rarely visualized on inspection. Special attention should be made for varicose veins, ganglion cysts, and bone spurs in the area as these can cause increased pressure in the tarsal tunnel. After inspecting, examiner should palpate the region carefully feeling for any obvious masses or tendon hypertrophy.
Motor Testing
The lateral plantar nerve innervates the abductor digiti minimi muscle and the medial plantar nerve innervates the abductor hallucis muscle. These two muscles can atrophy and weaken from nerve compression at the tarsal tunnel. These muscles can be evaluated in tandem by asking the patient to splay their toes outwards and assessing the tension of the abductor hallucis and abductor digiti minimi muscles. The strength can subsequently be assessed by asking patient to abduct great toe and 5th toe, and then resist examiner as examiner tries to adduct the great toe and 5th toe, rating the strength on the MRC grading system of 0-5.



Strength Assessment of Abductor Hallucis and Abductor Digiti Minimi: Patient abducts great toe and 5th toe, and then resists adduction from examiner squeezing toes together. Examiner can also use other hand to palpate muscle tension of the abductor hallucis and abductor digiti minimi.
Sensory Testing
Assess the sensory distribution of the tibial nerve using a rating system of 0 to 10, with 0 being no feeling at all and 10 being normal sensation. First, have patient close their eyes. Then, pick a location where patient has no complaints of sensory disturbances (like the shin) and lightly stroke the area with your finger, instructing the patient that if this sensation is 10 out of 10, please tell me from 0 (being no sensation at all) and 10 (being this sensation) how each of the following areas feel. Proceed to lightly stroke the plantar surface of the foot, noting regions of decreased or abnormal sensations.
Provocative Maneuvers
Similar to carpal tunnel syndrome, symptoms of tarsal tunnel syndrome can be elicited with provocative maneuvers that aid in clinical evaluation.
Tinel’s Test
Sensitivity: 58% [3]
Specificity: Not Reported [3]
Tinel’s test of the ankle is performed by tapping (either using fingers or reflex hammer) the tibial nerve directly over the flexor retinaculum posterior to the medial malleolus. The test is considered positive (Tinel’s sign) if patient reports paresthesia or numbness in the distribution of the tibial nerve or its branches. Note that occasionally the paresthesia can radiate proximally towards the calf, called Valleix phenomenon [4].

Tinel’s Test for Tarsal Tunnel Syndrome: Test is positive (Tinel’s Sign) if patient reports paresthesias, pain, or numbness in the distribution of the posterior tibial nerve or its branches.
Triple Compression Stress Test
Sensitivity: 85.9% [5]
Specificity: 100% [5]
The triple compression stress test is the most specific provocative maneuver and was designed to increase pressure in the tarsal tunnel by combining plantarflexion with inversion and simultaneous digital pressure [7].

Triple Compression Stress Test: Place patient’s foot in full plantarflexion and inversion with one hand, while simultaneously applying digital pressure over the tarsal tunnel just posterior to the media malleolus for 30 seconds. The test is considered positive if patient reports new paresthesia, pain, or numbness in the posterior tibial nerve or its distal branches in the foot [5].
Dorsiflexion/ Eversion Test
Sensitivity: 97% [6]
NOTE Sensitivity depends on what symptoms patient reports:
Numbness: 25%
Pain: 57%
Tenderness at Posterior Tibial Nerve (Area of Tarsal Tunnel) 97%
Specificity: 100% [6]
The dorsiflexion/ eversion test is performed by passively stretching patient’s ankle into maximum dorsiflexion followed by maximum eversion, and then maximum extension of the toes at the metatarsophalangeal joints. This position is held for 10 seconds to put maximum stretch on tarsal tunnel to increase pressure on tibial nerve. Immediately after releasing the position, the examiner should palpate the flexor retinaculum and ask the patient if they feel any tenderness in the area of palpation, or pain/ numbness in the toe, ball of foot, or heel. The test is considered positive if patient develops any of the above symptoms [6].


Dorsiflexion/ Eversion Test: Patient’s foot is placed in maximal dorsiflexion and eversion with maximal extension of the MTP joints for 10 seconds. Immediately afterwards, examiner palpates the flexor retinaculum overlying the tarsal tunnel and assesses for point tenderness or any paresthesias/ numbness in the distal foot.
Plantarflexion/ Inversion Test
Sensitivity: Unknown
Specificity: Unknown
Plantarflexion and inversion of the foot are both known to increase compartmental pressures, leading to the creation of the plantarflexion/inversion test [7].

Plantarflexion/ Inversion Test: Performed by placing the foot into maximal plantarflexion and inversion and holding for 10-15 seconds before returning the foot to neutral. The test is considered positive if patient develops pain or paresthesia in distal branches of the posterior tibial nerve.
Tarsal Tunnel Compression Test (Durkan’s)
Sensitivity: Unknown
Specificity: Unknown
The tarsal tunnel compression test is performed by applying pressure directly over the flexor retinaculum for up to 30 seconds to aggravate symptoms of tarsal tunnel syndrome. The test is considered positive if paresthesia, numbness, or pain develops in the tarsal tunnel or the distal branches of the tibial nerve in the foot.

Tarsal Tunnel Compression Test: Examiner presses firmly over the flexor retinaculum for up to 30 seconds or until symptoms develop. Test is considered positive if paresthesia, numbness, or pain develop in tibial nerve or distal branches in the foot.
Sources
1.) Nelson, Scott C. “Tarsal Tunnel Syndrome.” Clinics in podiatric medicine and surgery vol. 38,2 (2021): 131-141. doi:10.1016/j.cpm.2020.12.001
2.) McSweeney, Simon C, and Matthew Cichero. “Tarsal tunnel syndrome-A narrative literature review.” Foot (Edinburgh, Scotland) vol. 25,4 (2015): 244-50. doi:10.1016/j.foot.2015.08.008
3.) Schwieterman, Braun et al. “Diagnostic accuracy of physical examination tests of the ankle/foot complex: a systematic review.” International journal of sports physical therapyvol. 8,4 (2013): 416-26.
4.) Merriman L, Turner W. Assessment of the lower limb. 2nd ed. London, UK: Churchill Livingstone; 2002.
5.) Abouelela, Amr A K H, and Abeer K Zohiery. “The triple compression stress test for diagnosis of tarsal tunnel syndrome.” Foot (Edinburgh, Scotland) vol. 22,3 (2012): 146-9. doi:10.1016/j.foot.2012.02.002
6.) Kinoshita, M et al. “The dorsiflexion-eversion test for diagnosis of tarsal tunnel syndrome.” The Journal of bone and joint surgery. American volume vol. 83,12 (2001): 1835-9. doi:10.2106/00004623-200112000-00011
7.) Trepman, E et al. “Effect of foot and ankle position on tarsal tunnel compartment pressure.” Foot & ankle international vol. 20,11 (1999): 721-6. doi:10.1177/107110079902001108
Key Learning Points
- Learn anatomy
- Learn motor testing
- Review provocative maneuvers
Related to Tarsal Tunnel Exam
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam