What's the cause of this
skin finding?
July 6, 2017
Andrew Gilman, MD
Case Presentation:
This 30-year-old woman was admitted to our inpatient hematology team for neutropenic fever after recent induction chemotherapy for AML. She had been doing well on supportive therapy and broad spectrum IV antibiotics until she developed a worsening fever and hypotension. During resuscitation, the above diffuse vesicular rash appeared, covering most of her body surface. Concern was raised for disseminated varicella, given her profound immunocompromised state and lack of response to antibiotics, and she was started on IV acyclovir in addition to her previous broad spectrum antibiotics. What is the diagnosis?

Figure 1 - Patient's back with gloved finger for scale. (Image from Stanford Medical Center Case)
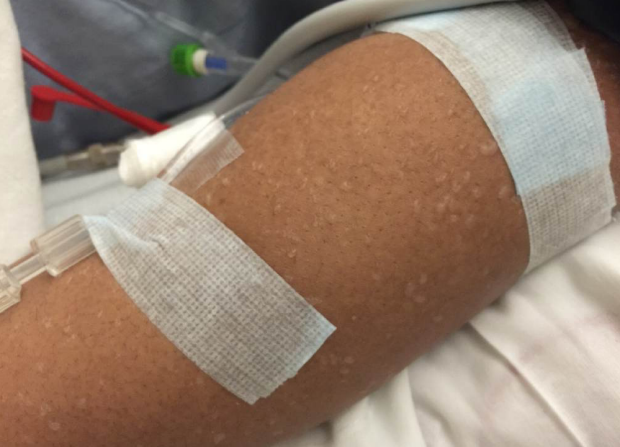
Image 2 (Image from Stanford Medical Center Case)

Image 3 (Image from Stanford Medical Center Case)
Diagnosis: Miliaria Crystallina
What is miliaria?
Miliaria is a dermatologic manifestation of occluded eccrine sweat glands. Two features are needed for development of the rash: an anatomical blockage of the duct and a stimulus for sweat production. There are three main subtypes: crystallina, rubra, and profunda. Miliaria crystallina involves the stratum corneum, producing clear vesicles without erythema. Rubra is localized deeper in the epidermis leading to leakage of sweat and resulting in inflammation, giving this subtype its characteristic erythematous papules (Figure 5). Profunda is deeper yet, often at the junction between the dermis and epidermis, and is most often seen after recurrent episodes of rubra.
Most commonly seen in children, it is often referred to as “heat rash” or “sweat rash”. Underdeveloped ducts in neonates combined with environmental exposure that induces sweating is the most frequent etiology. Certain drugs and sequelae of skin infections have also been implicated in producing the necessary anatomic abnormality.
In the image of our patient (Figure 1), note the lack of surrounding erythema, clear fluid, and eventual lack of crusted lesions. These can help distinguish miliaria from infectious etiologies. The initial, well-formed vesicles can be seen on the right side of the image while the later stage flaccid, ruptured vesicles are pictured on the left.
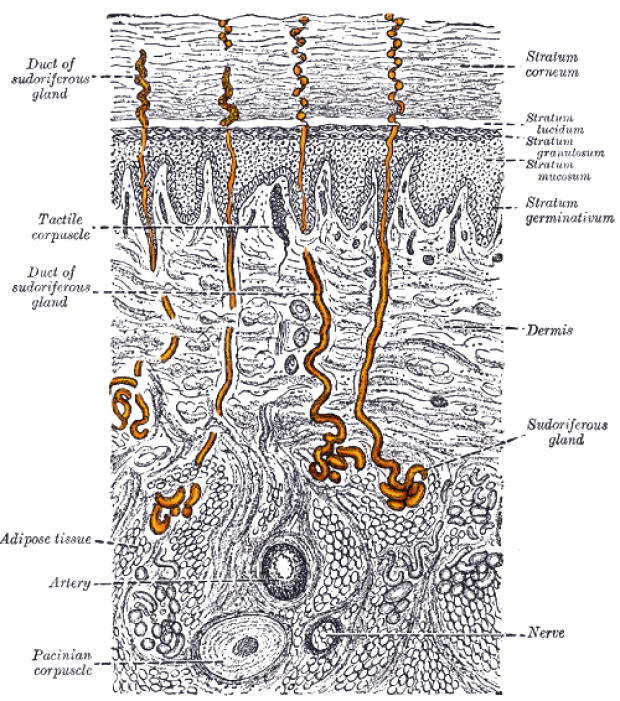
Image 4 - Sweat gland anatomy

Figure 5 - Miliaria rubra (Image credit: Wikipedia Commons)
How common is miliaria crystallina?
It is particularly common in neonates, with estimated incidence at approximately 9%1, reflecting a higher prevalence of anatomically underdeveloped glands in the young. It is less common in adults. As would be expected, the incidence is higher in humid or tropical climates.
What other tests should you order?
The diagnosis is a clinical one. While not necessary, a skin biopsy may demonstrate a vesicle within the stratum corneum of a sweat duct for crystallina.
What is the treatment and prognosis?
Miliaria crystallina is expected to resolve without intervention and without long term sequelae. Prevention of recurrence is aimed at treating the underlying cause, which is usually either environmental exposure or, as in our patient, fever. The rash is typically asymptomatic and requires no intervention. Significant symptoms associated with it should prompt investigation into alternative etiologies.
The exception is miliaria rubra, which may lead to pruritus and bacterial superinfection. These can be treated with topical corticosteroids and antibiotic ointments, respectively.
How did our patient do?
In our patient, it was postulated that rapid fluid resuscitation lead to localized edema, and combined with her uncontrolled fever, lead to the above vesicular rash. Her rash resolved over the following few days and can be seen in the at various stages in Figure 1. She had no recurrence during her hospitalization. Ultimately, she also recovered from her infection as her counts began to normalize.
Reference:
1. Hidano A, Purwoko R, Jitsukawa K. Statistical survey of skin changes in Japanese neonates. Pediatr Dermatol. 1986;3(2):140-4.