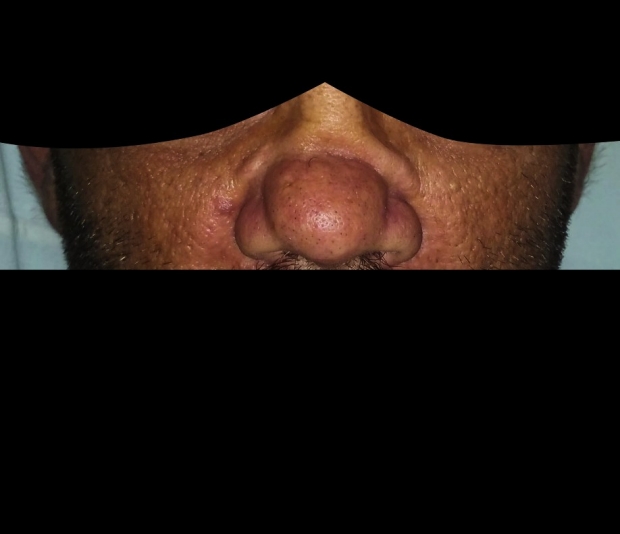
What’s the diagnosis? Patient presents with chronic sinusitis and this finding…
September 16, 2015
What’s the diagnosis?
Answer Below…
Answer: Granulomatosis with Polyangitis: aka, GPA. Diagnosis is based on the saddle nose deformity in a patient with severe sinusitis.
What conditions are associated with saddle nose?
1. Granulomatous Disorders:
a) Granulomatosis Polyangitis
b) Infection (Mycobacterial, Leprosy)
c) Sarcoidosis
2. Neoplastic Conditions, i.e. EBV Associated Nasal Lymphomas
-Lymphatomatoid Graulomatosis (B-Cell)
-Extranodal NK/T-Cell Lymphoma, Nasal type (T-Cell)
*Note: The above conditions are collectively called “Midline Destructive Disease”
3. Relapsing Polychondritis
4. Primary Atrophic Rhinosinusitis
5. Congenital Syphilis
6. Iatrogenic/Man-made
-cocaine abuse
-trauma (most common cause)
-surgery
-radiation
What is the underlying pathophysiology?
1. Inflammatory destruction of the nasal septum and boney sinus architecture, leading to collapse of overlying tissues. Seen in:
-Granulomatous Diseases
2. Coagulative necrosis of tumor cells and mucous glands and perivascular inflammation, leading to collapse of overlying tissues. Seen in:
-Lymphatomatoid Granulomatosis, NK/T-Cell Lymphoma
3. Vasoconstriction and ischemia, leading to collapse of overlying tissues. Seen in:
-cocaine abuse
4. Bacterial colonization of the nasal mucosa, leading to collapse of overlying tissues. Seen in:
-Primary Atrophic Rhinosinusitis
*Note: patients with Primary Atrophic Rhinosinusitis are predominantly colonized with Klebsiella Ozaenae (Ozaenae from the Greek term for “stench.”) The disease, most often seen in the developing world, presents with foul smelling nasal discharge.
-Other inflammatory chronic sinusitises (e.g., many GPA patients, like ours, are chronically superinfected with bacteria due to disrupted sinus drainage)
5. Autoimmune Cartilaginous Destruction, with inflammatory destruction of underlying tissues. Seen in:
-Relapsing Polychondritis
What are the expected radiographic findings in these disorders?
These will vary by mechanism and chronicity. Early on, CT may reveal mucosal thickening throughout the paranasal sinuses and a prominence of the soft tissues of the turbinates. Later—i.e., by the time the nasal bridge begins to collapse—CT may reveal bony resorption of intranasal structures including: the inferior and middle turbinates, ethmoid bulla and uncinate process, and lateral nasal wall. This can lead to lateral enlargement of the nasal cavities (“empty nose syndrome”) or, conversely, hypoplasia of the maxillary and frontal sinuses.
What symptoms might accompany a saddle nose deformity?
In most cases, patients will experience facial pain, recurrent epistaxis, episodic anosmia, nasal purulence, and nasal crusting. Patients with systemic causes, (e.g., the vasculitides) may experience weight loss, fevers, or symptoms related to various, disease-specific end organ pathologies.
What treatments are available?
For local symptoms, nasal lavage is recommended to prevent formation of crusts and drying of the atrophic nasal lining. An antibiotic may be added to the lavage when the nasal wash or nasal discharge becomes persistently purulent. For sinusitis secondary to autoimmune disease, antibiotic decisions may be complicated by the need for concomitant immunosuppression.
Q: What is the classic triad of organs involved by Granulomatosis with Polyangiitis, or GPA?
– Lung (85% of patients – pulmonary infiltrates, nodules, hemoptysis)
– Kidney (77% – glomerulonephritis, focal segmental—>rapidly progressive/crescentic)
– Upper airway (92% – sinusitis, nasal disease, hearing loss)
– The joints, skin, thyroid, and central and peripheral nervous systems can also be affected.
Q: What are the associated pathologic findings in Granulomatosis with Polyangiitis, or GPA?
Necrotizing vasculitis of small arteries and veins, with granuloma formation. Remember: granulomas represent a Type IV (T-Cell mediated) Hypersensitivity reaction. They do not involve antigen-antibody immune complex deposition (as in Type III Hypersensitivity reactions). Hence GPA’s designation as a “pauci-immune” vasculitis.
But wait: aren’t there antibodies associated with Granulomatosis with Polyangitis?
Yes! Anti-Neutrophil Cytoplasmic Antibodies, or ANCA. More than 90% of patients with active GPA have antibodies against Proteinase 3 (PR-3), an antigen present in the azurophilic granules of neutrophils. Because these granules are seen diffusely throughout the neutrophil cytoplasm on immunofluorescence, the antibodies are called cytoplasmic, or, “c”ANCA.
How are cytoplasmic (i.e., intracellular) antigens affected by serologic (i.e., extracellular) antibodies?
Good question. According to Harrison’s: “When neutrophils or monocytes are primed by [inflammatory cytokines], Proteinase-3…can translocate to the cell membrane, where it can interact with extracellular ANCA.”
Isn’t there another kind of ANCA?
Right again! pANCA: antibodies against neutrophilic antigens localized to the perinuclear area of the neutrophil. The most clinically significant of these pANCA are directed against Myeloperoxidase (MPO), a protein in neutrophil lysosomes. Anti-MPO antibodies are found in 75% of patients with Microscopic Polyangitis—or MPA. The memorable association of MPO with MPA is nice, because almost nothing else about the small vessel vasculitides is easy to remember.
Take Churg-Strauss Syndrome: a third pauci-immune small vessel vasculitis which has much in common with MPA and GPA. Many Churg-Strauss patients have pANCA, as in MPA; but they also have granulomas, as in GPA. Churg Strauss produces trademark lesion in the nose—the one GPA-affected organ not involved by MPA. But these lesions are nasal polyps (as in Cystic Fibrosis or Allergic Asthma), and their pathology is completely different from that of GPA’s saddle nose. Namely, they are infiltrated by Eosinophils rather than T-Cells. For this reason, Churg Strauss Syndrome is also called Allergic Angiitis and Granulomatosis.
Doesn’t Granulomatosis with Polyangitis have another name too?
Granulomatosis with Polyangiitis used to be called Wegeners’ Disease. But it was named for a German pathologist, Friedrich Wegener, who during World War II worked in a medical office three blocks from the Jewish ghetto in Lodz, Poland, where other physicians conducted experiments on concentration camp prisoners. In his time at Lodz, Wegener was known to have “autopsied a prisoner with oxygen injected in his bloodstream in an embolism study.” According to a 2008 New York Times article, Wegener—unlike doctors who joined the Nazi Party simply to be allowed to practice—joined the movement in 1932, before Hitler took power.
Wow. How did such a jerk end up lending his name to such an interesting disease?
Here’s where it gets really interesting. Wegener’s name was made famous by Dr. Jacob Churg—a renal pathologist who, in 1952, first introduced the term Wegener’s granulomatous into the English medical literature. Dr. Churg, as you may have guessed, is the same Dr. Churg who characterized Churg-Strauss disease. He is also, ironically, an Jewish refugee from Eastern Europe, who relocated to the United States in 1936 as a young medical school graduate. Quoting a letter to the editor of the journal Chest, Wegener’s fame is “largely attributable to an eastern European Jew, who, had he not escaped to the United States, would certainly have been incarcerated in a ghetto, perhaps even the notorious Lodz Ghetto, where Dr. Wegener was dissecting victims just 3 years later in 1939!”
Q: Isn’t there another rare rheumatologic disease with a German-sounding eponym and complicated historical legacy?
A: Yes: Reactive Arthritis. Characterized by the clinical triad of Anterior Uveitis, Urethritis, and Polyarthritis—and the genius mnemonic “Can’t See, Can’t Pee, Can’t Climb a Tree”—Reactive Arthritis was formerly named for Dr. Hans Conrad Reiter, a senior Nazi official who, according to the same article, “left an [even] clearer trail of war crimes” than Wegener did.
Written by Matthew Stevenson, MD
Sources
1. Langford C, Fauci A. The Vasculitis Syndromes. In: Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Localzo J. Harrison’s Principles of Internal Medicine, 18th ed. New York, McGraw-Hill; 2012:2785-2801.
2. Feder B. A Nazi Past Casts a Pall on Name of a Disease. New York Times. http://www.nytimes.com/2008/01/22/health/22dise.html?_r=4&. Published: January 22, 2008 (Accessed on September 7, 2015)
3. Emmett M. To the Editor: On Wegener and the ACCP. Chest. 2007;132(6):2066. doi:10.1378/chest.07-2720. Published: December 2007. (Accessed on September 7, 2015)
4. Freedman A, Aster J. Clinical manifestations, pathologic features, and diagnosis of extranodal NK/T cell lymphoma, nasal type. In: UpToDate, Connor R (Ed), UpToDate, Waltham, MA. (Accessed on September 7, 2015)
5. Michet C. Pathology of relapsing polychondritis. In:UpToDate, Romain P (Ed), UpToDate, Waltham, MA. (Accessed on September 7, 2015)
6. Falk R, King T. Clinical manifestations and diagnosis of granulomatosis with polyangiitis and microscopic polyangiitis. In: UpToDate, Forman J (Ed), UpToDate, Waltham, MA. (Accessed on September 7, 2015)
7. DeShazo R, Stringer S. Atrophic rhinosinusitis. In:UpToDate, Feldweg A (Ed), UpToDate, Waltham, MA. (Accessed on September 7, 2015)