Approach to the Exam for Parkinson's Disease
Parkinson’s Disease is one of the most commonly diagnosed motor disorders. It is important to be familiar with the physical exam so that you can confirm the diagnosis and monitor how the treatment is benefiting the patient over time.
Introduction
Parkinson’s Disease Exam
The physical exam in Parkinson’s disease (PD) is essential both for making a diagnosis and following the patient over time. It consists of a series of tests and maneuvers that help us identify and evaluate the four main characteristics of the disease:
- Bradykinesia
- Rigidity
- Tremor
- Gait & Balance abnormalities
In order to make a diagnosis, we must observe bradykinesia plus either one of the other motor abnormalities. Once a diagnosis is made and the patient is started on treatment, it is important to check these four features at every follow up visit, so that we can gauge the treatment based on how the exam has changed over time.
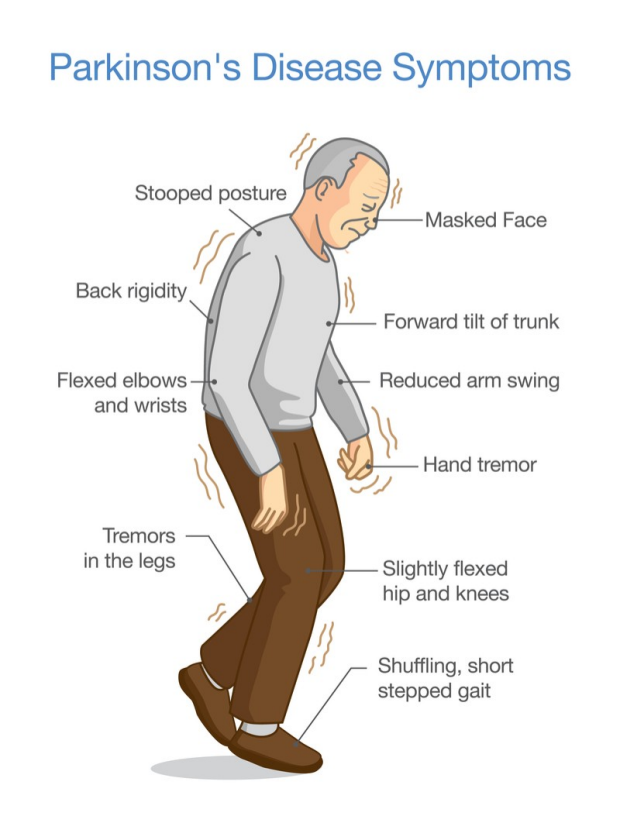
Some of the clinical features of PD. Image credit
Inspection
Parkinson’s Disease Exam
Before beginning the interactive part of the physical exam, it is very important to focus on observing the patients while they are giving the history, to notice any motor disturbances present at rest.
In particular we should focus on:
- Spontaneous movements, generally reduced in PD
- Hands gestures while talking, usually reduced or absent
- Eyeblink, whose spontaneous rate is reduced
- Resting tremor, usually affecting one hand only
- Fidgeting and crossing/uncrossing of the legs, that may indicate dyskinesia, a complication of chronic Levodopa therapy
It is important to remember that the inspection starts as soon as the patient walks in to the room.
Click this link to watch an example of spontaneous resting tremor on the video.
Bradykinesia
Parkinson’s Disease Exam
Bradykinesia is defined as a generalized slowness of movement, with patients struggling in particular with starting a movement. It is seen in almost every patient with Parkinson’s disease, making its presence essential for diagnosis. It is also one of the most debilitating symptoms of PD.
Rapid Alternating Movements
To test for the presence of bradykinesia we will have the patient perform rapid alternating movements. It is important to remember that these movements must be performed as fast as possible and as big as possible, meaning with the amplest range possible. All these tests are positive for bradykinesia if the range of motion and/or the speed reduce over time. For this reason, it is crucial to ask the patient to do at least ten repetitions for each movement.
Also, in both the upper and lower extremities, the movements more affected by bradykinesia are the finest ones, such as the movements of the toes and fingers.
Finger tapping
In finger tapping the patient is instructed to tap the index finger on the thumb as fast possible and as big as possible. This means that the patient should try to separate the two fingers as much as possible before tapping them. Make sure to test both the right and the left side.
Click this link to watch an example for the “finger tapping test ” on the video.

Finger tapping.
Fist Open Close
If the patient has arthritis of the hand joints, the finger tapping is not a very sensitive test. In this case, we can use other tests such as the fist open close. To perform this test, instruct the patient to open and close the fist as fast as possible and by spreading the fingers as much as possible.
Click this link to watch an example for the “fist open close test” on the video.
Rapid opening and closing of the fist.
Pronation/Supination of the Hand
This represents another alternative to the finger tapping test. The patient is instructed to flex the shoulder forward at 90° and fully extend the forearm. From this position, ask the patient to rapidly alternate pronation and supination of the hand. Again, look for a reduction in the speed and amplitude of movement, no matter how slight this is.
Click this link to watch an example for the “pronation/supination test” on the video.
Rapid pronation/supination of the hand.
Toe Tapping
It is possible to test for bradykinesia in the lower extremities too, where the most sensitive test is toe tapping. In this test the patient sits on a chair with both feet on the ground. The patient is instructed to rapidly tap the floor with the toes while the heel is kept in touch with the ground. The test is positive if the speed and/or amplitude of movement reduce over time.
Click this link to watch an example of the “toe tapping test” on the video.
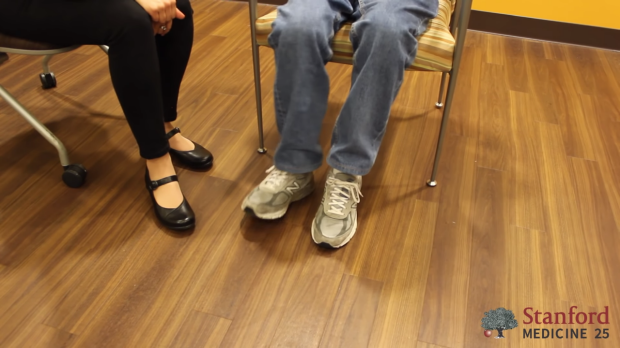
Fast toe tapping on the ground.
Heel Tapping
To carry on the test, first the patient has to sit on a chair with the feet on the ground. Then, instruct the patient to repetitively and rapidly tap the whole foot on the ground. This maneuver tends to be less sensitive than toe tapping. Again, the test is positive if the speed or amplitude of movement reduces over time.
Click this link to watch an example for the “heel tapping test” on the video.

Fast tapping of the heel on the ground.
Rigidity
Parkinson’s Disease Exam
Rigidity is defined as increased resistance to passive movement about a joint. It usually starts on one side and later spreads to the other one. It is similar to spasticity since both conditions show increased resistance to passive movement. However, rigidity is not direction dependent, that means there is the same amount of resistance both in extension and flexion of the affected limb. Also, rigidity is not velocity dependent, meaning that the tone does not change based on the speed of passive motion.
Passive Manipulation of Limbs
To test for the presence of rigidity, we need to passively manipulate the limbs of the patient. However, If the disease is in its early stage or the symptoms are well controlled with medications, we may not be able to see rigidity. We will need to use some activation maneuvers, that basically consist in performing repetitive movements with the limb contralateral to the one that is being tested.
Also, there are two types of rigidity:
- Lead-pipe rigidity: where the tone is uniformly and smoothly increased throughout the entire range of movement
- Cogwheel rigidity: where a tremor is superimposed on the hypertonia, making the movement irregular due to intermittent increase and reduction of tone
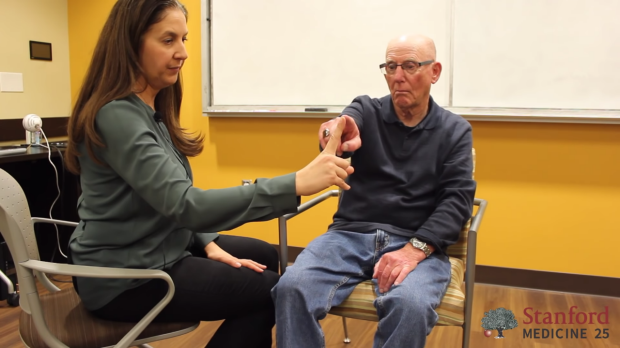
Upper Extremity Testing
For the upper extremity the most sensitive joint where to check for rigidity is the wrist. To uncover rigidity, passively rotate the wrist and feel for a resistance to the movement. It is very important that the arm of the patient is fully relaxed when rotating the wrist. To do this, place your proximal hand under the patient’s forearm, while your distal hand grabs and rotates the wrist of the patient. When rigidity is present, the range of motion will be preserved but you will feel a resistance in performing the movement.

Wrist rotation with activation maneuver.
It is also possible to test for rigidity in the elbow by passively flexing and extending the forearm.
In both cases, we can unmask the rigidity by asking the patient to forcefully and repeatedly tap the other hand on the knee as activation maneuver.

Elbow flexion-extension with activation maneuver.
Lower Extremity Testing
To test for the presence of rigidity in the lower extremity, place your top hand under the patient’s knee to fully support the weight of the leg and make sure the extremity is relaxed. Then, grab and rotate the patient’s foot with your bottom hand to test the ankle joint. After that, always by grabbing the patient’s foot, passively flex and extend the knee.
The activation maneuver in this case is identical to the one used for the upper extremity. The patient will tap his contralateral hand on his other knee.
Again, rigidity is present if a resistance, rather than a limitation to the range movement, is noted.

Passive rotation of the ankle.

Passive flexion-extension of the knee.
Tremor
Parkinson’s Disease Exam
Tremor is defined as an involuntary trembling of a body part. There are three main types of tremor:
- Resting tremor
- Action (Kinetic) tremor
- Postural tremor
All of these types of tremor can be seen in Parkinson’s disease, even though resting tremor is the more frequently observed one and also the most severe when all three tremors are present in PD.
Patients with essential tremor, instead, classically have more severe postural and kinetic tremors as compared to resting tremor.
Resting Tremor
In Parkinson’s disease resting tremor most commonly manifests in the hands as a rotatory movement of the fingers, especially the thumb and index (pill-rolling). Even though we could observe a resting tremor while the patients are giving the history, sometimes they may assume a position that suppresses the tremor. For example, they could sit on their hands or hold them in their lap. The best position to uncover a resting tremor is with the patient sitting on the chair with both hands lying relaxed on the thighs.
Click this link to see an example of resting tremor on the video.

Resting tremor on the left hand.
Postural Tremor
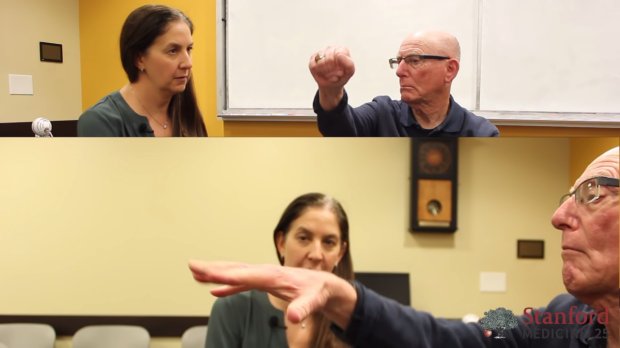
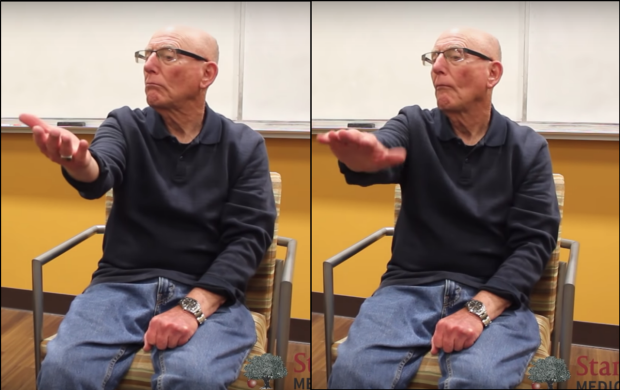
Postural tremor is a type of tremor that emerges when the patient maintains a position against gravity. To test for postural tremor, first have the patient fully extend the elbow and flex the arm forward at 90°. Then, ask the patient to spread the fingers out as much as possible and hold this position for a few minutes. This is necessary since a postural tremor in PD is often evidenced only a few seconds or minutes after the position in assumed.
Click this link to see an example of postural tremor on the video.

Position to test postural tremor.
Kinetic (Action) Tremor
Action or kinetic tremor is a type of tremor that is uncovered only when the patient is carrying out a movement. To test for kinetic tremor we can use the finger to nose test. In performing this test, the patients are instructed to alternatively touch their nose and our finger. In doing so, the patients should stretch their arm completely and should not move too fast. In this way we have more chances of triggering the tremor.
There is a different variant of the finger to nose test, in which the finger of the examiner changes position every time that the patient tries to reach it. This variant of the test is used to test for ataxia, rather than for tremor.
Click here to jump to the section of the video showing how to perform the finger to nose test.
Finger to nose test: the patient reaches for the finger of the examiner.

Finger to nose test: the patient goes back to his nose.
Gait & Balance Abnormalities
Parkinson’s Disease Exam
Patients with Parkinson’s disease can develop an alteration of the postural reflexes that causes instability in gait and balance control. Such alterations usually develop later in the course of the illness and are a major cause of disability, especially because of the high risk for falls that derives.
Using the exam to pick up postural instability is of the utmost importance for the management of patients with PD, since it will trigger either a medication adjustment or a physical therapy intervention both aimed at falls prevention.
We have three tests for this part of the PD exam:
1) Standing up from a chair
2) Free walking
3) Provoked “pull test” maneuver for balance
Standing From Chair
In this test we want to see if the patient is able to stand up from the sitting position without using the hands. To perform the test, first ask the patient to cross the arms on the chest and then to stand up. Make sure to keep one of your hands behind the patient’s back throughout the test, in order to prevent the patient to fall backwards and hit the head against the wall. In normal conditions the patients will be able to stand up without any difficulties.

Standing from chair (1): the patient crosses his arms on the chest.

Standing from chair (2): the patient stands up while the examiner keeps a hand on his back.
Free Walking
This part of the exam consists in observing the patient’s gait. To increase the chances of picking up any abnormalities that may be present, the patient should walk back and forth several times, ideally, in a hallway at least 10 feet long.
While the patient is walking, we need to look for:
- Loss of balance on the turns
- Reduced step length
- Loss of heel strike
- Loss of arm swings
These are typical abnormalities of gait in Parkinson’s disease. Also, in the initial stages of the disease, these anomalies tend to be unilateral, making them easier to recognize.
A gait with short steps and absent heel strike bilaterally is called “festinating” or “shuffling” gait and is typical of Parkinson’s disease.
Click here to see an example of festinating gait in the video.
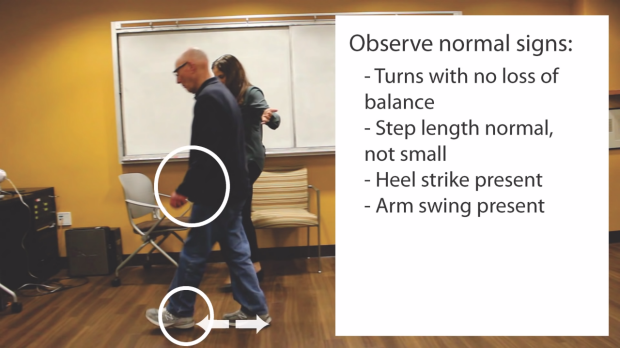
Observe for arm swinging, step length and heel strike.
"Pull Test" for Balance
In this test the examiner stands behind the patients and by pulling on their shoulder tries to make them fall backwards. If the patients are able to correct their center of gravity in just one or two steps, the test is negative for a balance abnormalities. The test is instead considered positive if the patients catch their balance in more than two steps or if they do not stabilize at all and tend to fall to the ground.
Click here to see an example of how the “Pull Test” should be performed.
To make sure the test is performed in a safe way, there are some precautions that should be taken:
- First, there should be a wall behind the examiner, so that if the patients do not manage to correct their balance and fall backwards, the examiner can grab them and together they can fall on the wall;
- Second, the examiner must teach the patients how to perform the test and must explain what is going to happen if they are going to lose balance and fall.
Click here to see an example of an abnormal result on the “Pull Test”.

Negative Pull Test.
Clinical Pearl
"When during a follow up visit we notice new worsening bradykinesia, tremor or rigidity, this does not necessary imply that a change in the medication regimen is needed, unless it is significantly impacting the quality of life of the patient. On the other hand, even the slightest impairment of gait and balance control necessitates an intervention, that may be as simple as physical therapy."
Key Learning Points
Learn the Parkinson's Disease exam aspects that include:
- inspection
- bradykinesia
- rigidity
- tremor
- gait and balance abnormalities
Related to Parkinson's Disease Exam
The Stanford Medicine 25
- Ankle Brachial Index
- Ankle and Foot Exam
- Aortic Regurgitation Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Dermatology Exam: Nevi (Mole) Exam
- Diastolic Murmurs Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Disease, Head to Foot
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Parkinson's Disease Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Pupillary Responses
- Rectal Exam
- Shoulder Exam Tutorial
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Visit the 25