Internal Capsular Stroke
A stroke in the internal capsule has unique clinical findings different from a stroke anywhere else in the brain. Those findings are reviewed here.
Introduction to the Exam for Internal Capsular Stroke
The internal capsule, a white matter structure, is a unique location where a large number of motor and sensory fibers travel to and from the cortex. Damage of any kind in this location will cause some relatively unique findings that can allow you to localize the lesions to the internal capule by exam alone.
Anatomy of the Internal Capsule
Location
The internal capsule is one of the subcortical structures of the brain.
Subcortical structures: internal capsule, caudate, putamen, globus pallidus, thalamus, brainstem
The anterior limb of the internal capsule separates the caudate nucleus and lenticular nucleus
The posterior limb separates the thalamus and lenticular nucleus
Types of fibers
- Anterior limb: frontopontine fibers (frontal cortex to pons), thalamocortical fibers (thalamus to frontal lobe)
- Genu (angle): corticobulbar fibers (cortex to brainstem)
- Posterior limb: corticospinal fibers (cortex to spine), sensory fibers
Blood Supply
- Anterior limb: mainly fed by the lenticulostriate branches of middle cerebral artery(MCA), less often branches of anterior cerebral artery (ACA)
- The lenticulostriate arteries are small penetrating blood vessels that supply blood flow to most of the subcortical structures.
- Genu: lenticulostriate branches of MCA
- Posterior limb: lenticulostriate branches of MCA & anterior choroidal artery (AChA) of internal carotid artery
Clinical Findings in Internal Capsular Stroke
Symptoms and Signs
Weakness of the face, arm, and/or leg (pure motor stroke)
Known as one of the classic types of lacunar infarcts, a pure motor stroke is the result of an infarct in the internal capsule.
Pure motor stroke caused by an infarct in the internal capsule is the most common lacunar syndrome.
Upper motor neuron signs
hyperreflexia, Babinski sign, Hoffman present, clonus, spasticity
Mixed sensorimotor stroke
Since both motor and sensory fibers are carried in the internal capsule, a stroke to the posterior limb of the internal capsule (where motor fibers for the arm, trunk and legs and sensory fibers are located) can lead to contralateral weakness and contralateral sensory loss
.gif)
If a patient has weakness +/- sensory deficits, how can you tell whether the stroke is subcortical or cortical? What other symptoms or signs can help you localize the stroke to the internal capsule as opposed to the cortex?
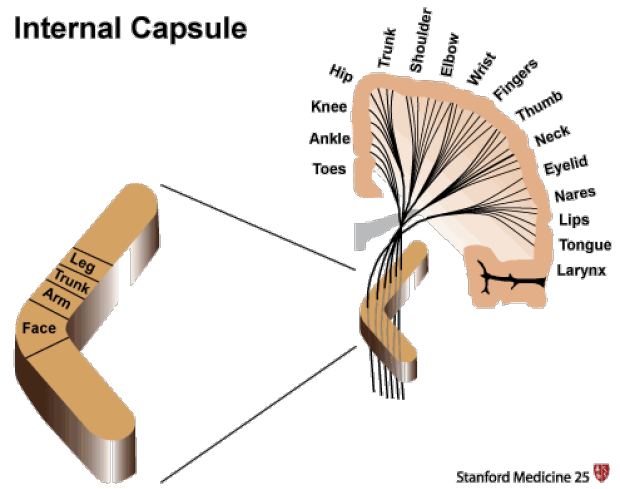
A patient who presents with arm and leg weakness may have either a small internal capsule stroke or a large ACA + MCA cortical stroke. Looking at the homunculus in the figure above, the cortical leg area is supplied by the ACA and the arm area is supplied by the MCA. However, the injury to the cortices produces other symptoms and signs that not commonly produced by injury to the subcortical areas.
The presence of these cortical signs may exclude an internal capsule stroke:
gaze preference or gaze deviation
expressive or receptive aphasia
visual field deficits
visual or spatial neglect
If any of these signs are present, the patient may have a cortical stroke, not an internal capsule stroke.
.gif)
Key Learning Points
- Know the anatomy of the internal capsule
- Know the clinical findings of an internal capsular stroke
Related to Internal Capsule Stroke
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam